Our personal plumbing system
Download printable version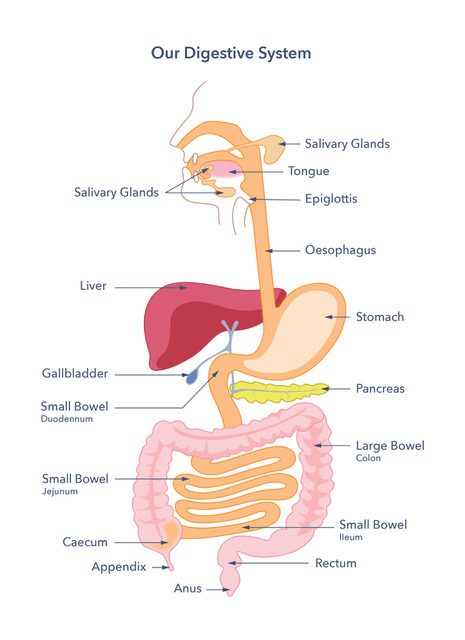
How does the gut work?
The gut is like a plumbing system. It has long, twisting pipes, valves, and fittings that connect to fixtures. Your mouth chews food to get it ready for digestion.
Mouth
The mouth works like a good waste disposal unit that breaks down rubbish, helping it move smoothly down the pipe. Eating slowly and chewing your food well help it move into the gullet (oesophagus) in smaller, easier-to-handle pieces.
Stomach
When food gets to the stomach, liquids like digestive juices are added. These include acid, which helps break down the food and starts digestion. There are also digestive enzymes in the stomach called pepsin and lipase. These enzymes continue the digestion of proteins and fats. The stomach muscles also create a ‘churning’ effect to help with digestion. The stomach has two sphincters, or “valves.” A sphincter is a ring of muscle with the ability to contract (close) and relax (open). The sphincters control how fast food moves through it. The lower oesophageal sphincter is a valve found where the oesophagus meets the stomach. The other valve is the pyloric sphincter. You can find this at the stomach exit where it meets the small intestine.
Small bowel
After all the chewing and churning, plus contact with digestive acid, the food barely looks like food anymore. This is when the stomach allows its contents to pass into the small bowel (intestine). The small bowel is long and narrow, allowing it to handle digested material from the stomach. Its width is why we call it the ‘small’ bowel. In an adult, the small bowel averages just over 6 metres in length and has three parts. The duodenum is nearest to the stomach. Next comes the jejunum, and finally, there’s the ileum. It’s helpful to know they have different names since they do different jobs.
Pancreas
The duodenum curves as it leaves the stomach. The pancreas sits nearby and plays a vital role in digesting food. You may know that the pancreas regulates your sugar levels. It does this by producing insulin. Insulin can be affected in conditions such as diabetes. What you might not know is that the pancreas also makes digestive enzymes. These enzymes break the food down into smaller parts. The pancreas produces the right digestive enzymes based on the food’s macronutrients. Macronutrients are proteins, starchy carbohydrates, and fats. The pancreas then sends the enzymes into the duodenum. They help break down the nutrients for absorption into your blood through the small bowel wall. Most nutrients are taken into the bloodstream at the jejunum of the small bowel.
Liver and gallbladder
Once in the blood, the nutrients go to the liver. The liver is a very important organ and has many functions. One of these functions is to manage nutrients in the blood, ensuring they nourish the body. The insulin produced by the pancreas helps with this too.
While many nutrients enter the blood from the small bowel, fats need extra help to be absorbed. The liver helps by making bile. This substance is stored in the gallbladder, a small sack under the liver. When food contains fat, the gallbladder releases bile into the duodenum. Bile attaches to fat in liquid food, breaking it into smaller droplets. It’s like adding soap to oil. This lets pancreatic enzymes break down fats into smaller pieces. Now they can attack the tiny droplets easily. Bile is useful because it also helps absorb some vitamins. But, like many things in the body, it works best when it’s in the right place. The body recycles the bile as it is absorbed back into the blood and returns to the liver for reuse. This takes place in the ileum, the last section of the small intestine.
Large bowel
When it leaves the small bowel, food is a thin, unappetising soup. But the large bowel is waiting eagerly for this soup. The small bowel is connected to the large bowel (or colon), which has a shorter, wider gut section. The large bowel hosts important occupants – the gut microbes (or microbiome). Gut microbes can eat a food component we have not yet mentioned, fibre. The small intestine can’t absorb fibre from food, no matter how crushed up it is. But our gut microbes thrive on it. Bacteria can sometimes use food that has slipped past your small bowel into your large bowel. This can include starch, sugars, and bits of protein, but they prefer fibre. It seems that the ‘friendliest’ bacteria prefer fibre. We know little about the microbiome. This makes it an exciting area of research. The gut microbes in the large bowel use the leftover food residue from digestion. The large bowel absorbs water and salts from the mixture. Over the course of a couple of days the mixture thickens and dries until it forms into poo (stools or faeces). The time for this to happen varies between individuals. Poo eventually reaches the rectum and is expelled through the anus. The anus is a sphincter that contracts and relaxes, letting poo pass through. Check out Guts UK’s PooTorial to see what is normal.
As you can see, the process of food digestion and absorption along the gut is complex. The body’s internal ‘plumbing’ system is helped by a complex network of blood vessels that are part of the circulatory system. These blood vessels carry nutrients from the gut to the body and help keep the gut healthy. Another consideration is the immune system, which has a whole army of special cells and molecules. They work together to protect the body from harmful invaders. The nervous system works with digestion by helping to control gut functions and movements. All these systems should work together in harmony.
What can go wrong?
With all this complexity in the gut, sometimes, things may go wrong. Consider the following steps in the digestion process.
- The way in which food moves through the gut.
- How the body breaks down food.
- How the body takes nutrients into the blood.
- The digestive system works with other body systems. Like the circulatory, nervous, and immune systems.
Starting at the top, swallowing may be faulty. This can cause coughing, choking and vomiting. Dysphagia is the term for this problem. It can happen due to issues with the muscles that help move food through or problems with the lining of the oesophagus. Issues with movement might come from a stroke or a degenerative disease that impacts the nervous system.
Oesophagus
A condition that affects the oesophagus is called achalasia. Food travels down the oesophagus through a process called peristalsis. Peristalsis involves wave-like muscle contractions in the oesophagus wall. As food reaches the lower oesophageal sphincter, the sphincter relaxes and opens. This allows the food to enter the stomach. When achalasia happens, the nervous system fails to send the signal to the muscles. This disrupts the wave-like motion and might stop the lower oesophageal sphincter from opening. As a result, the food can get stuck in the oesophagus.
The lining of the oesophagus can get damaged because of these events:
- Acid reflux.
- Eosinophilic oesophagitis is a condition where the immune system attacks the oesophagus, causing inflammation and tissue damage.
- Oesophageal cancer.
Some disorders make it hard for food to move down the oesophagus. Other conditions can cause the opposite issue. The lower oesophageal sphincter lets food enter the stomach. It also stops the stomach’s contents from coming back up the oesophagus. The inner stomach wall can handle the acid that breaks down food. But the oesophagus has a different lining that can get irritated by acid. Acid reflux, or gastro-oesophageal reflux disease (GORD), is a common complaint. It can cause heartburn, a painful burning feeling in the chest. Acid reflux can sometimes harm the oesophagus and lead to Barrett’s oesophagus. In a small number of people, this damage may lead to oesophageal cancer. Because of the higher risk of cancer, doctors keep a close watch on some people where the lining has changed (dysplasia). The goal is to catch cancer early if it develops.
Stomach
Sometimes, food has a hard time leaving the stomach after mixing with digestive fluids. It can struggle to pass through the pyloric sphincter. This sphincter opens and closes. It controls how quickly stomach contents move into the small bowel. Gastroparesis is a condition where the nerves and muscles that move the stomach don’t work properly. This means that the stomach might not churn the food properly, and/or the contents might not empty completely into the small bowel. This can lead to discomfort, bloating, nausea, and vomiting. It can also mess with blood sugar levels by tricking the pancreas into expecting food that doesn’t come. If the stomach dumps food into the small intestine too fast, it can trigger a condition known as dumping syndrome. This is usually due to gut surgery, but other causes can also be to blame.
The stomach and the first part of the duodenum have a common condition called peptic ulcers. These ulcers are quite uncomfortable. Their treatment has changed a lot in recent decades. Peptic ulcers were once believed to be caused by stress. Now, they are linked to a bacterium called Helicobacter pylori. Researchers in Australia found this link. Now, doctors use antibiotics and proton pump inhibitors to treat peptic ulcers instead of milk of magnesia. Peptic ulcers can also raise the risk of stomach cancer if the ulcer is in the stomach.
Another common condition that impacts the small intestine is coeliac disease. People with coeliac disease react to gluten, which is in wheat, barley, and rye. This reaction damages the small intestine’s lining and makes it hard to absorb nutrients and vitamins. Other conditions, like Crohn’s disease or small intestinal bacterial overgrowth (SIBO), can stop nutrient absorption. But this usually affects one or a few specific nutrients.
Other conditions that can affect the small bowel are:
- Ulcers
- Adhesions
- Blockages
Issues with small bowel movement include chronic intestinal pseudo-obstruction (CIPO). This happens when there’s no blockage. But problems with blood levels, nerves, or muscles can lead to unusual gut movement.
Pancreas and gallbladder
Pancreatitis is a painful inflammation of the pancreas. It can lower the production of pancreatic enzymes. This affects how nutrients are broken down and absorbed in the small intestine. Gallbladder issues can impact the small intestine. This disrupts bile flow, which is needed to absorb fats. The gallbladder can form stones, known as gallstones. These stones might block the bile duct, which connects the gallbladder to the small intestine (duodenum). The problem can happen if the valve, or sphincter, that controls bile flow into the small intestine isn’t working right. Doctors call this condition biliary sphincter disorder. It was once called sphincter of oddi dysfunction. In bile acid diarrhoea, bile acids aren’t reabsorbed by the small intestine. So, they move to the large bowel, leading to diarrhoea.
Large bowel
Many conditions can affect the large bowel. One of these is Inflammatory Bowel Disease (IBD). This group of diseases causes inflammation and ulcers in the bowel. Crohn’s disease can affect the whole gut, from the mouth to the anus. Ulcerative colitis and microscopic colitis are two types of IBD. They are only found in the large bowel. The large bowel can form pouches known as diverticula. This condition is common and is called diverticular disease. These pouches usually show no symptoms or discomfort. They can sometimes get inflamed or infected. This can cause complications known as diverticulitis.
Another common large bowel issue is irritable bowel syndrome (IBS). People with IBS feel cramp-like pain and have abnormal bowel movements. These include diarrhoea, constipation, or sometimes both, in turns. The causes of IBS are unclear. But food poisoning or gastroenteritis may trigger it. Doctors know IBS as a disorder involving the communication between the gut and the brain. Doctors call this a ‘disorder of the gut-brain interaction’ (DGBI). Nerves send information from the brain to the gut. This helps the gut function properly. In IBS, a communication fault leads to the symptoms. Nerves can be sensitive to normal bowel movements. This sensitivity causes pain. Doctors call it visceral hypersensitivity.
Many other disorders impact gut-brain interaction. Functional diarrhoea and functional constipation also affect the large bowel. Another example is functional dyspepsia, a type of gut-brain disorder that affects the oesophagus. These disorders can affect different parts of the digestive system.
The large bowel can also develop polyps, small growths on the wall of the bowel. Polyps are usually benign, which means they are non-cancerous. But some can turn malignant (cancerous) and may lead to bowel cancer. Bowel screening with the Faecal Immunochemical Test (FIT) is important to do. This test could find bowel cancer at an earlier stage when it might be more treatable. Many other diseases affect the gut and its related organs.
Liver
The liver helps with digestion, but overeating and drinking too much alcohol can harm it. People with a higher than healthy body weight can get metabolic-associated steatotic liver disease (MASLD). Research links this metabolic disease to fatty liver. It happens when fat builds up inside the liver. Drinking too much alcohol mainly causes liver damage and leads to alcohol-related liver disease (ARLD). Both conditions can worsen over time, causing liver fibrosis and, in the end, cirrhosis. The liver can regenerate and replace damaged tissue with new cells, but this ability isn’t endless. Chronic damage from things like excessive alcohol, viruses (like hepatitis), or some drugs can set back regeneration. This can cause scarring (fibrosis) and severe, irreversible harm (cirrhosis). This prevents the liver from functioning properly.
Cirrhosis can lead to ascites, which is a buildup of fluid in the abdomen. A swollen abdomen can lead to a poor appetite, constipation, and indigestion. It may also cause people to feel sick (nausea) or be sick (vomiting). Cirrhosis can also sometimes lead to liver cancer.
Our digestive system works hard to keep us healthy. It can only use the food we provide, so it’s important to maintain a balanced diet. The digestive system is complex, and it works with other body systems. This makes it possible for many things to go wrong. Figuring out the causes of some digestive issues can be tricky and take time. Taking care of your gut is important. This means watching what we eat, keeping a healthy weight, and checking for any signs or symptoms. Addressing any issues early can be helpful.
Discover more


Copyright © 2026 Guts UK. This leaflet was published by Guts UK charity in May 2026 and will be reviewed in May 2029. The leaflet was written by Guts UK and reviewed by experts in the digestive system and its effects on the gut and has been subject to both lay and professional review. All content in this leaflet is for information only. The information in this leaflet is not a substitute for professional medical care by a qualified doctor or other healthcare professional. We currently use AI translation tools on our website, which may not always provide perfect translations. Please check for further explanation with your doctor if the information is unclear. ALWAYS check with your doctor if you have any concerns about your health, medical condition or treatment. The publishers are not responsible or liable, directly or indirectly, for any form of damages whatsoever resulting from the use (or misuse) of information contained or implied in this leaflet. Please contact Guts UK if you believe any information in this leaflet is in error.