Overview
Crohn’s disease is a condition that causes gut inflammation. It is an Inflammatory Bowel Disease (IBD), alongside ulcerative colitis. Crohn’s disease occurs when parts of the gut become inflamed. Symptoms include diarrhoea, abdominal pain and tiredness. Inflammation can range from mild to severe. Severe cases may need strong medicine or even surgery.
Crohn’s disease is a lifelong condition. Prevalence is equal between genders. It can be detected at any age but is commonly diagnosed in adolescents and young adults under the age of 30.
Causes
Crohn’s disease affects 1 in every 650 people. The specific cause is unknown, but several factors are linked to the condition. Such factors include gut bacteria, lifestyle and diet.
Genes play a part in the development of the disease. About one-fifth of people with Crohn’s disease will have a family member also affected. Changes in genes controlling the gut’s immune response to microbes are linked to Crohn’s disease development. Identical twins of individuals with Crohn’s disease have a 1 in 4 chance of developing the condition. This shows that genetics alone do not determine the occurrence.
Environmental factors have a significant impact on the development of Crohn’s disease. A westernised diet has an influence. This diet is low in fibre, fruit and vegetables and high in sugar and saturated fats. High intake of food additives such as emulsifiers may be a factor. Another contributor may be Vitamin D deficiency. This is more common in countries in the northern hemisphere. It is unclear whether a Vitamin D deficiency leads to the development, or whether Crohn’s disease increases the risk of Vitamin D deficiency.
Weakened immune system functioning can contribute to the development of Crohn’s disease. This can be caused by stress. Smoking is another risk factor. The use of oral contraceptives is associated with an increased risk of development. All these possible causes need more research.
How does Crohn’s disease affect the body?
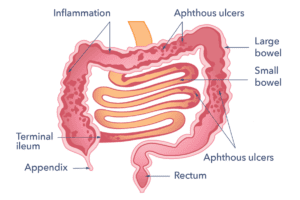
In most people, Crohn’s disease results in patches of bowel inflammation with groups of small sores (aphthous ulcers). These are similar to mouth ulcers, but can occur anywhere in the gut. In moderate or severe cases, ulcers become large and deep with a lot of nearby inflammation.
Inflammation causes redness, swelling and pain. This can cause the gut wall to thicken. This may narrow the inside of the gut, preventing food passing through. Sometimes, deep ulcers break through the bowel wall causing infection outside the bowel. This is called an abscess. If the infection doesn’t heal, or it heals but leaves a channel, a fistula can form. Fistulas connect the bowel to other areas. Fistulas are common around the anus. Scar tissue may form as the body recovers. This can lead to a narrowing in the bowel (a stricture). Sometimes, a stricture can cause a bowel obstruction. Strictures can also form because of previous episodes of inflammation in a part of the bowel.
Any part of the gut, from the mouth to the anus, can be affected. The most common area is the end of the small bowel (terminal ileum) through to the large bowel (or ‘colon’). The mouth, gullet or stomach is occasionally affected. In some people, only the large bowel is affected, which can resemble ulcerative colitis. The gut inflammation can sometimes trigger irritation outside the bowel. This can lead to ‘extra intestinal’ symptoms like arthritis and swollen joints, sore red eyes, or skin rashes.
People with Crohn’s disease can experience periods of remission when the disease activity is low. Flare ups occur when symptoms are stronger, and the disease is active. Treatment aims to achieve and maintain remission.
Diagnosis
Crohn’s disease can be difficult to diagnose because the symptoms can mimic those of other conditions. The diagnosis methods have improved in recent years. When you visit your GP with symptoms, the doctor must decide if further tests are necessary to rule out Crohn’s disease.
The doctor will listen and ask about any symptoms. They might also inquire about any medicine taken, recent travel abroad and if there is anyone in the family with a gut disorder. A physical examination may be performed. The doctor might feel the abdomen for signs of inflammation, tenderness or a lump. They might check whether there are any indicators of illness such as looking pale or underweight. A blood test may be arranged to detect any signs of inflammation.

If Crohn’s disease is suspected, the doctor may refer you to a specialist or request a stool sample. This will be tested for a protein called calprotectin, which is an indicator of Crohn’s disease. Further medical tests may be carried out such as:
Colonoscopy
This is the most commonly used test for diagnosing Crohn’s disease. During a colonoscopy, a thin, flexible tube connected to a camera is inserted through the anus into the colon and sometimes through to the end of the small bowel. This provides a detailed image of the bowel’s lining. The doctor may take a biopsy for further examination if needed. A biopsy is a small sample of tissue. Laxative preparation is needed before the examination. This will clear the bowel contents and allow for a better view of the bowel wall. Sedation is often given to minimise discomfort during the test. If the colon and last part of the small bowel appear normal, Crohn’s disease is unlikely to be present.
If the whole bowel needs to be examined there are several options including:
Magnetic resonance imaging (MRI)
The person is placed inside a machine that generates detailed images of the inside of the body. This enables the assessment of the structure and function of the gut. Sometimes a drink is consumed first to enhance visualisation of the bowel.
Capsule endoscopy
A capsule containing a tiny camera is swallowed, transmitting pictures as it travels through the bowel.
Barium follow through
Liquid barium is swallowed, and X-rays are taken as it passes through the bowel. Scans such as ultrasound or CT scanning may also be needed, especially if an abscess or external bowel problems are suspected.
How can Crohn’s disease affect you?
The effects of Crohn’s disease can vary between people, depending on the nature and severity of the condition. For many people, the condition does not significantly affect everyday life. For others quality of life can be affected. This is particularly true when experiencing fatigue and unpredictable flare ups. Living with Crohn’s disease might mean changing some aspects of your life. Learning about your condition can help you to improve your confidence. Preplanning with the help of your healthcare professional or IBD team can also help.
Symptoms
Diarrhoea, abdominal discomfort, mouth ulcers and joint pain are common symptoms. Blood or mucus may be present in the poo, especially when the lower bowel is affected. The body may be unable to absorb food which can trigger unwanted weight loss. Discomfort from symptoms can also induce weight loss through avoidance of eating.
The bowel contents can build up in narrowed and ulcerated areas of the gut. In some cases, the bowel may become blocked. This induces severe abdominal pain, bloating and vomiting. If this occurs, seek urgent medical attention.
Crohn’s disease can lead to complications that affect nutrient absorption. This can lead to fatigue due to low iron levels in the blood and side effects from medicine. Crohn’s disease can lead to low mood and sleep problems. People can feel unwell and have night sweats. If you or your child have any of the above symptoms or your child is not growing as fast as you’d expect, contact your GP.

How will Crohn’s affect me over time?
People with Crohn’s disease are more likely to have certain micronutrient deficiencies. These include vitamin B12, vitamin D folate and iron . This can affect energy levels and increase risk of deficiency disorders such as osteoporosis . This is thought to be linked to difficulty absorbing nutrients. Living with Crohn’s disease can take some getting used to, but a ‘normal’ life can often be led.
Severe cases can have a significant impact on daily life. A weak response to treatment can involve frequent flare ups. This makes symptom-free remission difficult to achieve. As there is no cure for this condition, it can relapse intermittently. Flare ups are triggered by various factors including stress, poor diet, missed medicine or other illnesses. These triggers will be unique to each person. When it is at an active stage, symptoms can make it difficult to cope with going out. Sometimes, people require time away from day-to-day commitments. However, treatment usually aims to improve symptoms within days or weeks and normal quality of life is restored.
Over time, most people learn how to manage their condition and avoid factors that may trigger flare ups.
Recurrence is twice as likely in smokers. Medicines including antibiotics and immunosuppressants may help to reduce the chance of recurrence. Doctors can prescribe these based on the individual’s risk.
Crohn’s disease does not significantly affect the chances of becoming pregnant. However, fertility can be affected in people designated female at birth by being underweight or malnourished. Plus, inflammation in the pelvis can occasionally affect fertility. Most medications for Crohn’s disease are safe during pregnancy, but methotrexate should be avoided. Other medications such as sulfasalazine can temporarily reduce male fertility. This is reversible when the medicine is no longer taken. Alterations to absorption in the gut means that Crohn’s disease can change the effectiveness of the oral contraceptive pill. It is always best to consult your doctor if you have Crohn’s disease and are planning a pregnancy or are already pregnant.

Treatment
The aim of any treatment for Crohn’s disease is to heal or reduce the inflammation. Some common treatments include:
Diet
Diet plays a role in managing Crohn’s disease. But there is no established diet specifically for the condition. It is suggested that a Mediterranean diet can decrease inflammation and improve symptoms. This diet is high in fruit, vegetables and healthy fats, and low in processed foods. It is very important that adequate calcium is consumed. This is because people with Crohn’s disease need more than the general population.

Exclusion diets without scientific evidence should be approached with caution. They could limit nutritional quality. Discuss any changes with your IBD team before implementing them. Generally, following healthy eating guidelines is recommended. There are situations where dietary changes can be helpful to ease symptoms:
- Strictures: This is a narrowing in the bowel. A reduction in fibre and indigestible foods can be helpful to reduce pain. Speak to your IBD team about seeing a dietitian who will be able to help.
- Diets for disease remission: Specialised liquid formula diets are used to treat Crohn’s disease. They are called either ‘elemental or ‘polymeric’ diets. These are usually used in children where maintaining growth and weight is critical. They are also used in adults who have the willpower to change their diet or where steroids need to be avoided. This involves taking a prescribed liquid diet to meet your nutritional needs. The diet excludes all other food/drinks except water for up to 8 weeks. It can be challenging to do. These diets rest the bowel, reduce inflammation, reduce symptoms and improve nourishment.
- Functional bowel symptoms: Some people have Irritable bowel syndrome (IBS), alongside IBD. This is when symptoms continue but there is no inflammation in the bowel. When this happens avoidance of specific dietary triggers may help to manage symptoms. Ask your IBD team for a referral to a gastroenterology dietitian.
- Unintentional weight loss: Speak to your IBD team to refer you to a gastroenterology dietitian if you are losing weight.
- Probiotics: There is currently no strong evidence for a beneficial effect of probiotic preparations.
Medicines
There are many medicines that the doctor may prescribe, depending on the persons situation. These are mainly aimed at the gut’s immune system and include:
- Antibiotics: Used to treat abscesses or to reduce the bacteria which ‘drive’ the inflammation. They are not used for long-term treatment. (e.g. metronidazole).
- Aminosalicylates: Commonly used to reduce mild inflammation in a similar way to aspirin. Aminosalicylates can minimise inflammatory flare ups and usually have no or only mild side effects.
- Steroids: Taken as tablets. They are stronger medications to suppress inflammation when the symptoms are more severe. They are often used as a first line therapy. Steroids are very effective (about 8 out of 10 people have a good response). Some can have side effects such as weight gain, insomnia, infection and acne. Prolonged use can result in bone weakening. A steroid called budesonide is now being used as it has less side effects than other steroids. Steroids are only used as a short-term treatment (e.g. 3 months) to establish remission.
- Immunosuppressive drugs: Used to reduce inflammation over a longer period. They can replace steroids. They are normally taken as tablets or injections. Azathioprine and mercaptopurine are prescribed most often. Around 2 out of 3 people respond well to them. They can take up to 3-6 months to become effective. Methotrexate is another immunosuppressive drug. This can be the next choice if azathioprine or mercaptopurine have failed. Most people tolerate the medications well.
- Biologics: Contain active substances. They can be used over longer time periods. Examples include infliximab, adalimumab, vedolizumab and golimumab. They are administered every 2 to 8 weeks by regular intravenous drip or injection under the skin. These treatments are very effective but can also induce side effects. Examples of these include increased rates of infection, joint pain and allergic reactions. Biologics are usually reserved for people with moderate to severe Crohn’s disease. Or prescribed when other treatments have not worked. This is because they affect the immune system. Hospital specialists must administer them. It is important that you discuss any concerns or questions with your IBD team.
A new method of giving infliximab and vedolizumab is by using injection pens that can be self-injected. This is currently in its early stages. People with Crohn’s disease, or their carers, can do it themselves in their home, which makes it easier to give.
- Small molecule drugs: Emerging oral (by mouth) medicines are under trial. These reduce inflammation by blocking key pathways. They include:
- JAK (janus kinase) inhibitors: Examples include tofacitinib filgotinib, upadacitinib .
- IL23p19 Inhibitors: Examples include guselkumab, risankizumab, mirikizumab .
More evidence is needed for their use in Crohn’s disease.
It is recommended that people with Crohn’s disease get the flu jab each year. This is because of potential suppression of the immune system.

Surgery
Surgical procedures can be a very important part of the treatment of Crohn’s disease. When drugs are ineffective, surgery can be required to remove thickened, obstructed parts of the bowel. The surgical removal of the affected section of bowel usually works well. There are generally few complications after surgery and full health is quickly restored. Surgery is also performed when badly affected parts of the bowel have caused an abscess or fistula in the abdomen. Occasionally, colonoscopy with special dilating balloons can be used to open up narrowed sections.
- Keyhole surgery: Keyhole surgery is also called a laparoscopy. It is less invasive than open surgery and means there is a shorter recovery time. A camera can be inserted into a small hole made in the abdomen. A common operation for Crohn’s disease is a right hemicolectomy (removing part of the right colon). This is usually performed to remove a narrowed terminal ileum.
- Open abdominal surgery: This is also called a laparotomy. This is a more traditional method of surgery. The doctor can see inside the abdomen without using a camera.
- Stoma surgery: Contrary to what many people believe, a stoma will often be temporary. A segment of the diseased bowel is removed. Then a very delicate join called an anastomosis is made between the ends of the bowel. To protect this join while it heals, the surgeon will then create a temporary stoma. It is then taken away at a second, smaller operation a few months later. A colostomy is where the end stoma is formed from the large bowel. An ileostomy is when the stoma is formed from the small bowel. This is more common when someone is under-weight or taking steroids. Both of these situations reduce the ability of body tissues to heal.
Support
What to ask your doctor?
- Is my Crohn’s disease well controlled?
- What monitoring do I need?
- Please can I have the contact details of the IBD team?
- Is my steroid intake being kept to the minimum?
Where can I get more information?
There are many organisations around for those who suffer from Crohn’s disease.
CCUK is the UK’s leading charity working on Crohn’s disease and other forms of IBD.
Crohn’s In Childhood Research Association (CICRA)
CICRA is the UK’s only children’s IBD charity, providing support and information for young people and their families and funding research to find improved treatments and ultimately a cure.
The IBD Standards say what high-quality care should look like at every point of a patient’s journey – from first symptoms, to diagnosis, treatment, and ongoing care.
IBDesis have created a fantastic video explaining IBD in South Asian languages.
Research
Scientists are working hard to understand Crohn’s disease. They do lots of important research. But there are still many things they don’t know for sure. The James Lind Alliance helps decide which questions about health are the most important to study. This is called a priority setting partnership. People who have Crohn’s disease, their helpers, and researchers came up with a list of the top 10 questions they want answering. Crohn’s and Colitis UK, is funding a priority setting partnership. They’re looking into how technology can help people with Crohn’s disease, especially young people.
There’s also an organisation called the National Institute for Health and Care Excellence (NICE). NICE gives advice to health care professionals about how to take care of people. They have a list of questions they want to find answers to about how to help people with Crohn’s disease. The list is found in their guidance for managing Crohn’s disease. This list gets updated a lot because new information comes in all the time. Guts UK are also proud to support research into Crohn’s disease.
Discover more:



Copyright © 2026 Guts UK. This leaflet was published by Guts UK in 2024 and will be reviewed in 2026. The leaflet was written by Guts UK and reviewed by experts in Crohn’s disease and has been subject to both lay and professional review. All content in this leaflet is for information only. The information in this leaflet is not a substitute for professional medical care by a qualified doctor or other healthcare professional. We currently use AI translation tools on our website, which may not always provide perfect translations. Please check for further explanation with your doctor if the information is unclear. ALWAYS check with your doctor if you have any concerns about your health, medical condition or treatment. The publishers are not responsible or liable, directly or indirectly, for any form of damages whatsoever resulting from the use (or misuse) of information contained or implied in this leaflet. Please contact Guts UK if you believe any information in this leaflet is in error.