Dave’s story – Oesophageal cancer
I asked: "And if I don’t have the surgery?" They said: "Six to nine months. That’s all you’ve got." It was one of those decisions you haven’t got a choice to make. I had to go for it.
Tell us about you
“My name is David. Everyone calls me Dave. I live in Bognor Regis, close to the beach. I’m married, with two daughters, two grandsons, and a granddaughter. I’m 71 this year. I worked in print before retiring, and now I’m a full-time volunteer in patient advocacy.”

Can you describe when your symptoms started and what they were?
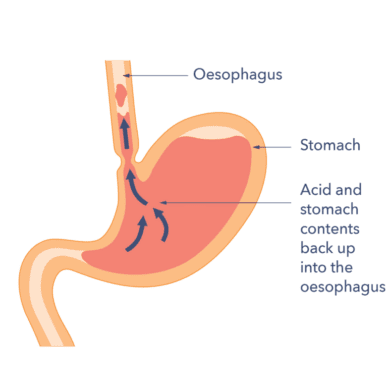
“I’d had heartburn, reflux, and indigestion for a long time. I put it down to everyday life like stress, work, or maybe that curry I ate. I’d take PPIs (a type of medicine that helps in managing the symptoms of heartburn and reflux) for a few months, and it would clear up, but really, it was just masking the symptoms. Like most people, I thought it was normal.
The real red flag was when I started struggling to swallow. Food would get stuck, and I’d have to cough it back up. That’s when I knew that this wasn’t normal. I went to my GP, who initially said it was just heartburn but referred me for an endoscopy (a thin tube with a small camera on the end inserted via the mouth), just in case.”

Talk us through your journey with oesophageal cancer
“It all happened fast. I got a referral within two weeks, and by the time I saw the consultant, they were talking about surgery straight away.
I was diagnosed with oesophageal cancer and Barrett’s oesophagus at 52 years old. Back then, I was one of the youngest patients they’d seen. The tumour was at the junction of my stomach, and it was at a size where they could go straight in with surgery. The consultants told me it was a 10-hour operation with big risks. I asked: “And if I don’t have the surgery?” They said: “Six to nine months. That’s all you’ve got.” It was one of those decisions you haven’t got a choice to make. I had to go for it.

They removed 80% of my stomach and most of my oesophagus. Since diagnosis, I dropped from 14 stone to 10 and a half stone. I couldn’t eat, couldn’t drink, and was in hospital for 15 days with a feeding tube to receive nutrition for my body. It changed everything. It goes against my previous 50 years of living and eating. I had to change.”
What happened after the surgery?
“Fifteen days after surgery, I was finally allowed to try eating. The first cup of tea and piece of cod and mashed potato were the best I’d ever had.
It took me three months before I felt ready to think about going back to work, but I was still weak, low in weight, and constantly tired. I returned part-time with my wife driving me, as I wasn’t able to drive yet. It took about six months before I was strong enough to return full-time.”
How are you now?

“Eating now is a lot different. I have to graze throughout the day, having five or six small meals instead of the usual three. This brings its challenges. You can’t always find time at work for an extra meal, but it’s gotten better over time. I can now eat almost anything but in smaller amounts.
One issue I deal with is dumping syndrome. Certain foods, especially those with high sugar content can trigger it. It’s a lot of trial and error and sometimes it happens without warning. When it does, I often have to sit quietly, close my eyes and my body shuts down for a while to recover.
Since the surgery, I can’t lie down for two to three hours after eating. So, I plan my meals early in the evening to give the food time to move through my system before bed. It’s just something I’ve gotten used to.
Socialising has been one of the hardest parts. It’s tough when you’re the one with a small starter while everyone else enjoys a three-course dinner. You don’t realise how hard socialising becomes until you actually can’t do it.”
Why did you start a patient support group?
“When I was diagnosed, there was no local support group, and I wanted to talk to someone who had been through it. I wanted to know how to live and eat without most of my stomach. The hospital team was great, but until you hear from someone who’s been on that journey, it’s hard to know what to expect.
Three months after my surgery, I started a support group with the local hospital. The group is still running today, offering both face-to-face and virtual options to include people from other areas. It’s a space where people don’t have to worry about what they eat or drink. They can share their experiences and give hope to new patients, showing them they’re not alone.”
What do people often ask about oesophageal cancer?
“A lot of people wish they had been diagnosed earlier. The big question is always: “Why me?” Most people feel they haven’t done anything wrong. Many don’t smoke or drink. But oesophageal cancer can happen for many reasons, including genetics and the environment.
People frequently ask about how to eat for the rest of their lives, whether their stomach will ever grow or stretch, and when to stop eating. It’s practical advice they need, but it’s hard because everyone’s journey is different. While we have dietitians who can offer nutrition advice, the best we can do is share what worked for us. It’s trial and error, but it’s possible to adapt.”

What are your hopes for the future?
“I’d love to see my oldest grandson, who’s 15, get into university and pursue biology, maybe even research one day. Personally, I just want to live life to the fullest. Age is just a number. It’s about what you do and how you do it. For me, it’s about staying healthy, staying active, and doing what I can to help others along the way.”
Why do you support Guts UK charity and advocate for patient Involvement in research?
“As a patient advocate, it’s not only about helping others go through their journey but also speeding up research to improve survival rates. Raising awareness about symptoms, encouraging people to get checked, and educating GPs about early signs can all make a difference.
A key part of my passion is ensuring patients have a role in non-clinical research, where we can ask important questions and help shape treatments. We need the patient voice in research to guide better treatments and ensure that it truly meet patient needs.“
Guts UK is funding research into the deadliest digestive cancers to diagnose these cancers earlier, and save lives. Oesophageal cancer is one of the six less survivable cancers. The others are stomach, pancreatic, liver, brain & lung cancer, with an average five-year survival rate of just 16%.
We have joined forces with other charities to make up the Less Survivable Cancers Taskforce (LSCT). With the aim of increasing these survival rates to 28% by 2029. But we can’t do it without you.
You can save lives. Please consider donating today. Thank you.