Bile Duct Cancer
Download printable versionOverview
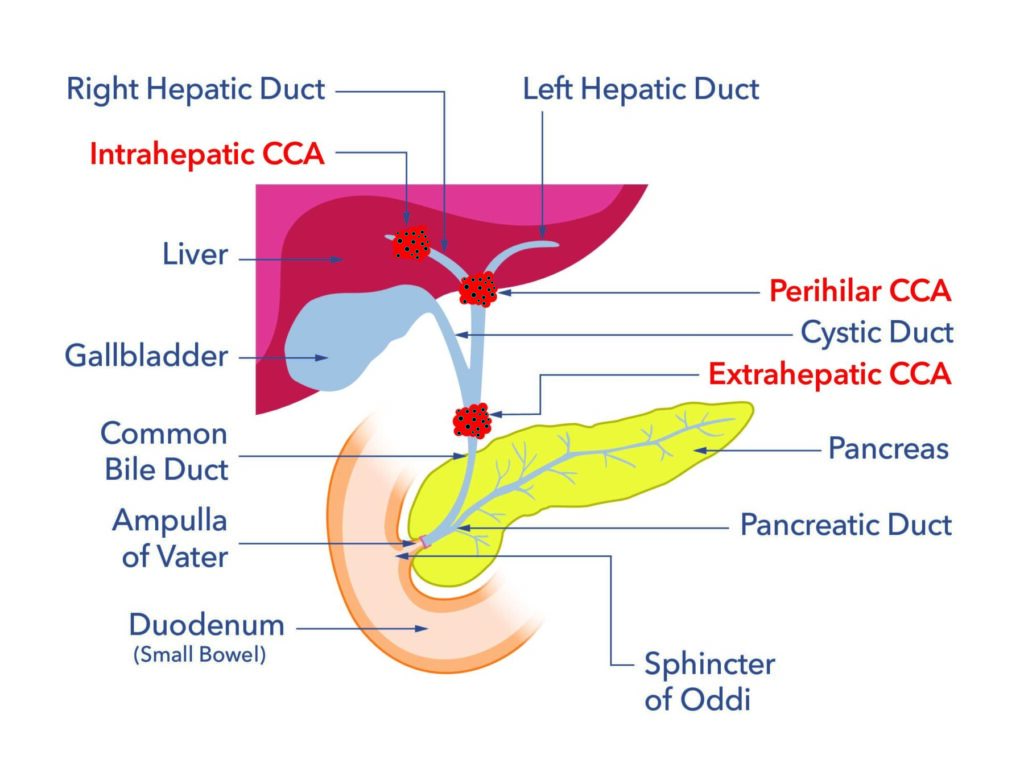
Cholangiocarcinoma, also known as bile duct cancer, is pronounced kol-an-gee-oh-car-sin-oh-ma. Cholangiocarcinoma is a cancer found in tubes called ducts. The ducts are found both inside and outside the liver and they carry bile that is made in the liver. Bile helps us digest fats from our food. Cholangio means bile duct and carcinoma means cancer. Cholangiocarcinoma is usually found in three places:
- Intrahepatic or iCCA. This means the cancer is found in the tubes inside the liver.
- Extrahepatic eCCA. This means the cancer is found in the tubes outside the liver.
- Perihilar or Hilar pCCA. This means the cancer is where the tubes from the liver join the tubes outside the liver.
Bile duct cancer occurs in both men and women equally. Slightly more men than women get cholangiocarcinoma inside the liver (iCCA). Most people are diagnosed after age 65. But 4 out of 10 people are under 65. It affects adults of all ages.
In the UK 2.2 per 100 000 people are diagnosed with bile duct cancer every year. This cancer is very rare. This number is like 24 people being diagnosed in a large city, the size of Birmingham. Cholangiocarcinoma seems to be on the rise in the UK. Researchers believe more people getting diagnosed with long term liver disease is the cause. Most people diagnosed with bile duct cancer do not have a family history of the cancer.
Causes
The cause of bile duct cancer in the UK is known for 3 to 4 in every 10 people. For the rest the cause is unknown. Where known the causes can include:
Age
Most people are diagnosed over 65 years of age.
Primary Sclerosing Cholangitis (PSC)
Primary Sclerosing Cholangitis (PSC) is an autoimmune disease of the bile ducts. It is the most common known cause of cholangiocarcinoma. The risk of a person with PSC developing bile duct cancer in their lifetime is between 1 in 10 and 2 in 10. This figure can vary depending on the source of the data. The cancer occurs more often in the first two years of being diagnosed with PSC. The risk falls after two years. For more information about PSC, see pscsupport.org.uk.
Chemical exposure
Thorotrast was a drug used as a contrast agent. It contained a radioactive compound, thorium dioxide. It was used to produce x-rays from the 1930s onwards. It is closely tied to bile duct cancer. Thorotrast was banned from use in the 1970s.
A chemical called propylene bichloride, which is used as a solvent also has a high risk. It is used in paint strippers, varnishes, and furniture finish removers. There is also a risk of developing cancer inside the liver (iCCA) with asbestos exposure. The risk is lower outside the liver (eCCA).
Cysts in the biliary system (Choledochal cysts)
Cysts in the bile ducts make bile duct cancer more likely. These cysts differ from the common liver cysts. Most liver cysts are harmless.
Cirrhosis of the liver
This can be a risk for developing bile duct cancer. This happens more in the biliary ducts in the liver (iCCA). It is less common in the bile ducts outside the liver (eCCA).
Chronic pancreatitis
People with chronic pancreatitis have a higher risk. They are at risk of developing cancer outside the liver (eCCA). This is thought to be caused by narrowing and inflammation of the bile duct. The cancer may develop around the area of inflammation.
Gallstones
Gallstones can get stuck in the biliary ducts for a long time. This raises the risk of bile duct cancer outside the liver (eCCA).
Other risk factors
There are several other risk factors, but these risks are lower. Examples are:
- Having inflammatory bowel disease.
- Having type 2 diabetes.
- Having stomach ulcers. The risk in stomach ulcers is suspected to be because of H pylori infection.
- Infections such as hepatitis B and hepatitis C. These carry a higher risk of developing bile duct cancer in the liver (iCCA) than outside (eCCA).
- People who have been diagnosed with Caroli disease. Caroli disease is a rare disorder of the bile ducts. People develop bile duct widening. They also may develop inflammation and stone formation. Caroli disease runs in families.
- Lifestyle risk factors include alcohol intake. This carries a risk of developing bile duct cancer inside the liver (iCCA) only. Other lifestyle risks include smoking and having an unhealthy high body weight.
- Infection with a liver fluke (parasite), often because of travel to east Asian countries.
Whilst the list above is long, it should be remembered that cholangiocarcinoma is still classed as a very rare cancer and most causes of it are unknown.
Symptoms
Symptoms can initially be vague and may include:
- Unintentional weight loss
- Loss of appetite
- Feeling tired or generally unwell
- Feeling sick
- Having symptoms of a fever such as high temperature and shivering
- Abdominal discomfort
- Indigestion

Depending on the site of development of the bile duct cancer it may produce jaundice. Signs and symptoms of jaundice include:
- Yellowing of the whites of the eyes and the skin (skin yellowing may be less obvious in people with darker skin types)
- Itching skin
- Dark coloured wee (urine)
- Pale coloured poo
Diagnosis
A GP may do several blood tests on the liver. The tests are called liver function tests (LFT). They can find problems with the liver or bile ducts. The GP may then refer you to a gut specialist or a liver specialist. The specialist will request further tests. The tests might include:
Ultrasound scan
This equipment makes sound waves. The waves create a picture of the liver, the biliary ducts, and nearby organs.
CT scan
This is a type of scan that uses X-rays. It can build a 3D image of the body’s insides.
MRI
This equipment produces a magnetic field. It can build a 3D image of the inside of the body.
Magnetic resonance cholangiopancreatography (MRCP)
This is a type of MRI scan that looks at the biliary ducts in more detail.
Endoscopic retrograde cholangiography (ERCP)
This is a thin tube with a camera at the end that is passed through the bile ducts. The doctor can inject a dye into the biliary tubes. It will show up on an x-ray (fluoroscopy) to identify any problems. If there is a narrowing, the doctor might insert a tube called a stent or blow up a tiny balloon inside the tube. It widens the narrowing and allows bile to flow into the digestive system. The doctor could take fluid samples to search for abnormal cells8. the doctor can also take biopsies for tissue analysis.
Endoscopic ultrasound scan (EUS)
This uses a thin tube to pass an ultrasound probe into the digestive system. This can produce a picture of the pancreas and its ducts. This scan also shows the doctor where to take a small tissue sample from for testing.
Percutaneous transhepatic cholangiography (PTC)
Percutaneous means ‘done through the skin’. This procedure involves injecting a dye with a thin needle. The needle goes through the skin. Then the needle goes into the bile duct within the liver. It could show any blockages. In the same procedure, the doctor may take tissue samples to analyse. A drain may then be inserted to drain the bile. This can help fix any jaundice. The drain can go inside or outside the body.
Positron emission tomography (PET)
This is a radioactive scan that detects active tissues in the body. The test can be used to detect cancer or to see if cancer has spread to other areas of the body.
Imaging tests may strongly suggest cancer but the only way to confirm it is by taking a small cell sample (biopsy). This is most often done during an ERCP.
Laproscopy
The doctor may also consider laparoscopy. Doctors use a small endoscope inserted through a small incision in the belly to visualise the area where they suspect cancer. Surgeons use general anaesthesia to perform it. Surgeons do the laparoscopy in the operating room.
What happens if cancer is found?
Staging shows if the cancer has spread to nearby organs or to other areas in the body. Staging helps guide tissue sample collection and treatment options. The doctor will use a system called TNM.
- T relates to the size of the main tumour.
- N is whether it has spread to the lymph nodes
- M is whether the tumour has spread to other areas of the body.
The system’s reporting will depend on where the tumour is found. Please see the link here for further information.
Treatment
Surgery to remove distal extra hepatic bile duct cancer
If the cancer is in the lower bile duct. Surgeons might recommend a type of surgery commonly called a Whipple’s procedure. Doctors call this procedure a pancreaticoduodenectomy. This involves removing part of the stomach and small bowel. It also removes the gallbladder, part of the pancreas and the affected bile ducts. It may also involve removal of the surrounding lymph nodes.
Contra-indications to surgery for bile duct cancer
It may not always be possible to have surgery. Some of the reasons surgery may not be possible are:
- The cancer has already spread to other parts of the body.
- The liver is damaged by scarring (cirrhosis).
- The person is not fit enough to recover well after the surgery.
The surgeon will explain the risks and benefits of surgery. This will help you can decide about whether to go ahead.
Liver transplant
Liver transplant is not routinely offered in the UK for bile duct cancer. A pilot study is underway. It will be suitable only for a small group of people, depending on the size and position of the cancer. Your cancer team can discuss this with you. They can say if a transplant might be right for you.
Chemotherapy
Chemotherapy uses medication that is swallowed or injected into a vein. It works inside the body to destroy cancer cells (cytotoxic). It can be used at various stages of treatment. But, it is most common for cancers not suitable for surgery. The goal is not to cure the cancer but to control its growth. This is called palliative chemotherapy.
Chemotherapy is sometimes used before surgery to reduce the size of the cancer. This may increase the chance of completely removing the cancer. This increases the chance of survival. This is called neoadjuvant therapy. Doctors may also use chemotherapy after surgery. It reduces the risk of the cancer coming back. This treatment is called adjuvant chemotherapy. There are various types of chemotherapy for bile duct cancer. You can read more about them at the AMMF website.
Newer cancer therapies treat cancer precisely. They are called targeted therapy. They are also called precision medicine. How the cancer responds to treatment may vary. It depends on the genetic type of the cancer, which varies from person to person. Recently, England, Wales, and Scotland approved a drug called pemigatinib. This treatment is for people who cannot have the tumour removed by surgery. It is either locally advanced or has spread to other parts of the body. Doctors use it when they find fibroblast growth factor receptor 2 (FGFR2) in the cancer cells. This receptor is identified by molecular testing. Pemigatinib blocks the FGFR2 receptor. This stops cancer from growing and spreading.
Another recent targeted therapy that has been approved is called durvalumab.
Stent insertion
A blocked or narrowed bile duct can be helped with a stent. It is a small, thin, and expandable tube placed in the duct. This widens the duct to allow bile to flow. This treatment can treat jaundice symptoms. Doctors usually do it before chemotherapy or surgery. The stents may be a temporary or a permanent treatment. They can block with debris over time so you may be recommended to have a stent change. Whether it needs changing also depends on the type of stent used.
If you have a stent and see the signs of jaundice (see above), contact your doctor or nurse.

How will I be monitored over time?
On diagnosis, you may meet a clinical nurse specialist (CNS). They will be your contact through treatment. The group of doctors, nurses, and other therapists who work together is known as the multidisciplinary team or MDT. This team will discuss the diagnosis and possible treatments for people with bile duct cancer. Your doctor or nurse will share the MDT’s decision with you. But the MDT in your local hospital may not carry out liver surgery for eCCA. The MDT then seek an opinion from a specialist liver surgical MDT in the region. You can find a list of centres here on the ammf.org.uk website. Contact us on 0207 486 0341 if you would like a copy.
Treatment of symptoms in palliative care
As a tumour advances, it grows through the wall of the ducts to invade nearby tissues. It can then spread to other areas of the body via the blood and lymphatic system. These are known as ‘secondaries’ or, more specifically, ‘metastases’. If the cancer has spread, treatment is often for symptoms and quality of life, not a cure.
Chemotheraphy
This is the main treatment used when the cancer can be no longer cured. There are several different options for chemotherapy. Sometimes, they use a mix of the chemotherapies. Your cancer team can advise which option is best for you.
Radiotheraphy
Radiotherapy uses high-energy waves, like x-rays. It uses them to destroy cancer cells. Radiotherapy may reduce cancer growth. It can also ease symptoms if the cancer cannot be cured.
Cholangiocarcinoma varies widely. So, doctors must consider treatment for each person. Doctors might consider:
- Other health issues.
- How well the liver is working.
- Past treatments.
- The size of the tumour, its blood supply and any involvement of bile ducts, blood vessels, bowel and chest wall.
Support
What to ask your doctor
- What treatment is best for me?
- Are there any specialist nurses? Can they help guide me through the diagnosis and treatment?
- Would I be able to be referred to a palliative care team if my cancer is not able to be cured?
- Can I be referred to a dietitian for advice? (Ask if you are struggling eating or losing weight.)
- Do I need to be referred to a specialist centre?
During treatment, you can often contact specialist nurses that can offer support too.

The charity that supports people diagnosed with cholangiocarcinoma is The Alan Morement Memorial Fund (AMMF). Click here to visit the charity’s website.
DISCOVER MORE:



Copyright © 2026 Guts UK. This leaflet was published by Guts UK in 2024 and will be reviewed in 2027. The leaflet was written by Guts UK and reviewed by experts in bile duct cancer and has been subject to both lay and professional review. All content in this leaflet is for information only. The information in this leaflet is not a substitute for professional medical care by a qualified doctor or other healthcare professional. We currently use AI translation tools on our website, which may not always provide perfect translations. Please check for further explanation with your doctor if the information is unclear. ALWAYS check with your doctor if you have any concerns about your health, medical condition or treatment. The publishers are not responsible or liable, directly or indirectly, for any form of damages whatsoever resulting from the use (or misuse) of information contained or implied in this leaflet. Please contact Guts UK if you believe any information in this leaflet is in error.