Overview
The medical term perianal disease means problems around the anus or back passage. The main conditions are explained on this information page. They are listed by the main symptom. Causes and treatments are listed under the disease name.
Causes
There are several causes of perianal disease. Please see the information below for individual diseases. Not all of them are avoidable. There are, however, some lifestyle factors that might help to prevent perianal disease. This includes having enough fibre and fluid in the diet to avoid constipation. Find out more about fibre here.
Symptoms
Perianal disease can cause one or a mixture of these symptoms:
- Itching
- Pain
- Lumps
- Bleeding
- Discharge – either fluid or pus
Diagnosis
Sometimes problems can be diagnosed ‘clinically’. This means you see a doctor or other clinician and they make a confident diagnosis without any special tests. This will depend on how long it has been going on and the pattern of your symptoms. First, it will be important for your doctor to take a history. This means going through the story of your symptoms in a structured way.
After this, a physical examination is usually carried out. When this is done, a doctor or other trained clinician will examine your belly (abdomen). They may also need to examine inside the anal passage. The information the doctor gathers will help plan the next steps. You can request a chaperone or a person of the same sex to undertake this examination.
Further tests may be required. These may include:
- Proctoscopy or rigid sigmoidoscopy. This can be carried out by a GP, advanced nurse practitioner (ANP) or by a specialist. It involves inserting an illuminated hollow plastic tube into the rectum through which air can be gently blown to enlarge the bowel and increase the amount of bowel lining which is visible. This allows the lining of the lower bowel and rectum to be searched for any lumps, ulcers or abnormalities. You may be given suppositories or an enema to clear the lower bowel immediately before the test. You will be given information about what to expect on the day of the test.
- Flexible sigmoidoscopy and colonoscopy: If your GP or advanced nurse practitioner (ANP) can’t find an explanation for your symptoms, they might refer you to a hospital or specialist centre. These places can examine a larger area of the bowel. Normally performed as a day case in hospital, they usually involve light sedation or nitric oxide (‘gas & air’). A long thin tube with a camera at the end (an endoscope or sigmoidoscope) is inserted into the rectum to look at the bowel and take small samples (biopsies). Sigmoidoscopes look at a small area of the large bowel whereas colonoscopes can look at the whole of the large bowel. You will be given information about how to prepare for the test. This might involve changing your diet on the days leading up to it. If you are a diabetic you can contact the endoscopy unit for more advice if needed. You will also be asked to take a bowel preparation medicine to clear your bowel. This is to enable the doctor to see the bowel wall more clearly. The bowel prep will cause diarrhoea, so you would be better to stay close to a toilet, once you have taken it.
Special X-rays such as a barium enema can examine the large intestine using X-rays and a white liquid called barium. An enema is the insertion of a liquid into your rectum through a small tube. The barium coats the lining of your bowel making it easier to see on X-ray. Preparation may be similar to the sigmoidoscopy or colonoscopy above.
Scans such as MRI or CT scan may be needed to give details of the surrounding anatomy (parts of the body) and help the doctor check that there no other problems.
Individual conditions
Information about individual conditions and their treatments can be foudn in this section.
Conditions with itching as the main symptom:
Pruritis ani
Itching around the bottom or pruritis ani can be caused by moisture such as sweat, soaps and shower gels. Rinse the area with a wet flannel or use a bidet or have a shower after having a bowel movement. Avoid using soap if possible but if soap is needed, use a small amount of non-perfumed soap sparingly. Pat skin dry and use a smear of petroleum jelly. If moisture is a problem, a tissue pad between the buttocks may help and if the skin is dry, certain moisturising creams could be tried. Carrying a pack of non-perfumed moisturised wipes to clean the anus to avoid scrubbing with dry tissue may be useful. Avoid rubbing too hard when using a towel and consider carefully using a hair dryer on a low setting to dry yourself after washing. These simple measures are usually effective, but if they do not help you, you should see your GP as there may be another cause. This could include an infection such as intestinal worms or candida (also known as thrush).
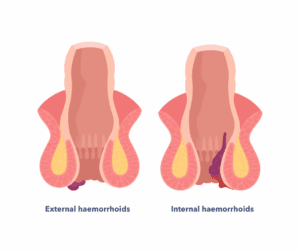
Haemorrhoids or piles
Haemorrhoids are blood vessels inside the anus that have become more swollen or have small tears. This can happen when we try to strain to pass stool (poo) or because of raised pressure in the lower abdomen. Women who are pregnant are at greater risk of getting haemorrhoids. This swelling may often cause a lump and the vessels may tear and bleed. The bleeding into the surrounding tissue can cause clots, resulting in pain.
Haemorrhoids may be internal or external. Internal are inside the anus. External piles protrude outside the anus.
The first treatment for haemorrhoids is to avoid constipation. This means making sure you are drinking plenty of fluids through the day and taking a healthy amount of fibre in the diet. Other treatments are creams and suppositories that reduce the pain or swelling. If these do not help, you should see your GP to discuss if you need to see a specialist for surgical treatment.
Surgical treatments for piles can include:
- Banding: This is where small flexible bands are placed around the base of the pile which cause them to wither and fall away.
- Injection: This is called sclerotherapy. It involves injecting an oily substance inside the swollen blood vessels of the pile which causes it to clot and shrink.
- Surgery: A number of different operations are available to remove or shrink piles that are either too large or prolapsing, making them unsuitable for banding. A surgeon could advise on which procedures are most suitable.
Conditions with pain as the main symptom:
Haemorrhoids
See information above.
Anal fissures
This is a split in the skin in the lower part of the anus. It often causes pain when passing stool (poo) and can cause bleeding. The pain can be severe and sometime people use expressions such as ‘feeling like passing broken glass’ to describe it. It affects about 1 in 350 people and is the second most common perianal condition after haemorrhoids to affect women during or after pregnancy. Anal fissure seems to affect men and women in similar numbers. They are most common between the ages of 18 and 35 years but can affect younger and older people.
What causes anal fissures?
In the past, anal fissures were often blamed on constipation and a tear being caused by passing hard poo. However, anal fissures may occur without constipation, and it may be linked with problems in the blood supply to the skin around the anus.
Anal fissures may also be caused by Crohn’s disease, infections and rarer disorders such as sarcoidosis, an autoimmune condition. There is also a link with certain medications such as nicrorandil (taken for angina heart pain) and chemotherapy. Don’t stop taking any medication without speaking to your doctor first they may be able to suggest an alternative.
How is a fissure diagnosed?
It can be diagnosed by clinical examination (see above). Sometimes, a specialised ultrasound scan is needed to check for problems of the anal sphincter. A test called anorectal manometry may be needed to assess the pressure inside the anus canal. A thin, flexible catheter with a small balloon is inserted into the rectum. You will be asked to squeeze the muscles, cough or bear down to help check if the muscles in your bowel are working correctly. Bowel preparation is not always required and your doctor will provide more information about the test.
How are anal fissures treated?
Simple measures such as taking the right amounts of fibre in your diet and a healthy fluid intake can help all people affected by anal fissures. This may be all that is needed for people experiencing this problem for the first time.
If symptoms continue, creams containing a medication called calcium channel blockers or nitrates may help. These work by relaxing the muscle of the anal sphincter.
If these treatments do not work, surgery may be needed. There are a number of different procedures that can help, and a surgeon could advise on which would be the best for you. One of the procedures involves an injection of botulinum toxin (such as Botox) to relax the muscle of the anal sphincter.
Perianal Abscesses
These are collections of pus around the bottom which result in extreme pain and tenderness in the area. They can be red, hot and swollen. People with abscesses may feel unwell with fevers and chills. If you have any symptoms like this, it is important to seek medical advice straight away as this could be early symptoms of sepsis. Sepsis is a widespread infection that needs urgent treatment. Sometimes an abscess will ‘burst’ and a smelly, sticky liquid (pus) may leak out which can bring some relief of the pain.
What causes an anorectal abscess?
Most abscess are caused by an infection of the small glands that are in the sphincter of the anus. These glands can become blocked leading to infection. They can also become blocked by conditions that cause inflammation such as Crohn’s disease.
How is it diagnosed?
Clinical examination (see above).
Sometimes a scan may be needed. This is usually only necessary if an abscess is deeper inside or thought to be caused by a more serious condition.
How can an anorectal abscess be treated?
Surgical treatment will sometimes be needed. The procedure is called incision and drainage. It involves making a small cut and letting the pus drain out. Antibiotics are not an alternative to surgery, but they may be given if any infection has started to spread.
Anal ulcer
This is a break in the skin or surface tissue of the anus that is not healing. This can cause pain and bleeding. This can be caused by inflammatory bowel disease such as Crohn’s disease, ulcerative colitis or ischemia (lack of blood supply to the bowel). Rarely ulcers deeper inside can be due to solitary rectal ulcer syndrome (SRUS).
You will need to see a specialist for these conditions; the treatment depends on the diagnosis.
Pilonidal disease
This is an inflammation in the skin in the cleft between the buttocks near the base of the spine that is caused by hair being forced under the skin by friction. The resulting inflammation can cause a cyst, an abscess (see above) or a sinus (a small blind channel into the skin). About 8 in 10 of people affected are men and it seems to affect mainly younger people.
How is it treated?
If there is painful swelling and/or discharge this usually means an abscess has formed and surgical treatment may be needed (see above). If there are no symptoms of pain, simple measures can help such as improved hygiene and avoiding sitting for long periods. Other measures that can help are hair removal and weight loss. If possible, avoiding prolonged sitting can help, but of course this is difficult for people in some jobs. Surgery may be necessary to remove the cyst or sinus.
Proctalgia fugax
Proctalgia fugax causes episodes of sharp pain in the anus which can come on suddenly. This seems to occur mainly at night or when resting without any obvious cause. Episodes last from a few seconds to up to half an hour and seem to go away as quickly as they come on. It is thought to affect up to 18 in 100 of the adult population. For most people, attacks of the pain are few and far between so many people do not see a doctor about it. There is no clear physical cause for proctalgia fugax.
If any pain carries on or attacks are happening more often it is important to consult a doctor to check that there is no other cause.
How is it treated?
Treatment is not usually needed but for the few people that have prolonged episodes, salbutamol inhalers can help. It is important to do this only with the advice of a doctor or other qualified prescriber.
Coccygodynia
Coccygodynia is a severe pain in the coccyx, the small bone at the very base of the spine. The coccyx is sometimes called the tailbone. The pain can be pulling and sharp in nature.
Who mainly gets it?
The average age of onset of coccygodynia is 40 years but it can occur at any age. About two thirds of cases are post traumatic (after an injury) the rest are idiopathic (which means no precise cause can be found) . Males are affected five times as often as females.
What causes it?
- After a fall onto the buttocks (the backside)
- After childbirth
- Conditions such as arthritis
- Rare causes are some types of infection
How is it assessed?
If coccygodynia does not settle with simple measures, x-rays or an MRI scan may be needed to exclude other causes of the pain.
How is it treated?
First treatment might include:
- Non-steroidal anti-inflammatory medications (such as ibuprofen)
- Shaped cushions
- Physiotherapy
If these do not help after a period of up to three months, other treatments may be needed. This might include an injection of steroid and local anaesthetic into the tissue or where the coccyx joins the spine. If injections or similar measures do not help after six months or longer, referral to a spinal surgeon might be needed. This is usually a Coccygectomy which means cutting away a part of the coccyx.
Conditions that cause bright red bleeding:
- Anal fissures – see above
- Haemorrhoids – see above
- Rectal cancer
- Inflammatory bowel disease – Crohn’s disease or ulcerative colitis, although Crohn’s disease doesn’t always cause bright red bleeding
Any bleeding from the anus should be brought to the attention of your GP. Please see our PooTorial for more information.
Conditions that cause lumps:
Skin tags
These are painless fleshy folds of skin found in the anal area. Sometimes they have been caused by other conditions such as prolapsed piles, anal fissures or inflammatory bowel disease and are usually diagnosed because of other symptoms such as pain or bleeding. Skin tags do not usually need any special treatment.
Warts
Warts are small lumps which are usually caused by a virus. The virus can be passed on by sexual contact but this is not always the case. If you suspect you have warts it is important to seek treatment in a specialist clinic for sexually transmitted diseases (STD clinic). Either your GP can refer you or in most areas you can contact the STD clinic yourself.
You can find more about sexually transmitted diseases and how to protect against them on the NHS website.
Anal cancer
This can present as a lump but can also cause bleeding or pain.
How is it diagnosed?
By clinical assessment. Usually, a biopsy will be done. An MRI and CT scan will be required to assess for any spread of the cancer.
How is it treated?
This could be combined treatment of chemotherapy and radiotherapy. Sometimes surgery may be required. Find out more at gutscharity.org.uk/bowel-cancer.
Conditions causing discharge:
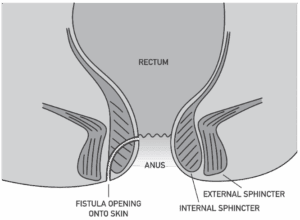
Anal fistula
An anal fistula is a small tunnel that forms between the inside of the anus and the surrounding skin. This can cause pain, irritation and smelly discharge. A fistula may also cause a lump near the anus. Some fistulae are complex and have more than just one channel.
What causes an anal fistula?
These are caused by a channel left behind after an abscess (pocket of pus) has drained. The end of the fistula may be visible as a hole or small lump in the skin close to the anus. Most anal fistulas are caused by infection in the glands around the sphincter muscles of the anus and may follow on from a perianal abscess. The minority of anal fistulas are caused by other conditions such as Crohn’s disease, hidradenitis suppurativa (a skin condition causing lumps), or infections such as TB. They can also occur after radiotherapy or chemotherapy treatment. Sometimes the fistula can form a channel into the vagina, see complex fistulas below.
How is it diagnosed?
Fistulas are diagnosed by clinical examination – see above. Often an MRI scan may be needed to determine the anatomy (path) of the fistula.
How are fistulas treated?
This depends on the type of fistula and where it tracks around the anal canal. You will need to be assessed by a specialist. Often the treatment is a surgical operation.
Here are a list of the main treatments. The descriptions here are very simplified. If you need a particular treatment your specialist will give you more advice. It is very important that when you have a discussion about this, you feel that you understand the risks and benefits of the procedure recommended for you:
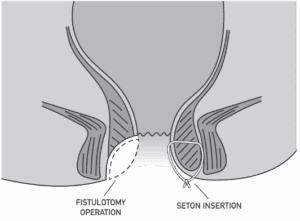
- Fistulotomy (laying open): This is the most common operation for anal fistulas. It is done by making an incision (a cut) along the length of the fistula so that it is open up and allowed to heal as a flat scar.
- Seton: A seton is a piece of surgical thread that is passed through the fistula. This keeps it open and allows it to drain. Other treatment will usually be needed after this.
- Advancement flap procedures: This involves cutting out the fistula and covering the end where it enters the anus with a flap of tissue taken from the anus or rectum. This procedure is done if the fistula passes through the anal sphincter and the surgeon wishes to avoid a fistulotomy which would involve cutting the sphincter.
- LIFT procedure (Ligation of the Intersphincteric Fistula Tract): This involves tying off and removing a piece of the fistula tract where it passes between the inner and outer sphincter muscles.
- Endoscopic ablation, or Video-Assisted Anal Fistula Treatment (VAAFT): A tiny camera is placed inside the fistula tract. The camera is used to look for branches of the fistula and a current can be used to burn the walls of the tract, cleaning it and hopefully allowing it to then heal.
- Laser surgery, or Fistula-tract Laser Closure (FiLaC): A small laser is passed along the fistula tract and laser energy is used to seal the fistula. Devices other than laser can be used to deliver energy to do the same thing, such as radiofrequency ablation (FISTURA).
- Bioprosthetic plug: A plug made of animal tissue is placed within the fistula tract to block the tract and encourage it to heal.
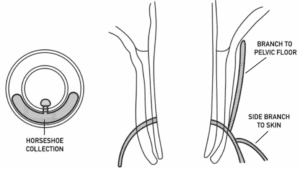
Complex fistulas
Some anal fistulas are complicated. They pass through both sphincter muscles and involve too much muscle for a safe fistulotomy. They are called trans-sphincteric fistulas. Surgeons prefer to do sphincter-sparing operations when trans-sphincteric fistulas happen. Sphincter-sparing operations are not as effective as a fistulotomy.
In women, vaginal fistulas are seen as complex. This is because the sphincter muscles are thinner in that area. Some complex fistulas have side branches or pus collections (abscesses) that don’t drain well. Surgeons call pus that forms a circular ring around the anus a horseshoe collection. Complex fistulas need initial treatment to drain the infection or close side branches. Then, a surgeon could perform an operation to help it heal.
Support
How can perianal disease affect you?
It’s often hard to figure out the problem from symptoms. So, if you notice bleeding, new pain, or lumps, ask your doctor for an assessment. In most cases, the GP can reassure you that the problem is harmless and easy to treat. For a few people, symptoms mean they need an urgent referral to a bowel specialist.
If you are experiencing faecal incontinence (bowel leakage), please see our information on faecal incontinence here.
If you have been diagnosed with Crohn’s Disease or ulcerative colitis you can find more information from Crohn’s and Colitis UK at crohnsandcolitis.org.uk. You can contact the charity by telephone on 0300 222 5700 or email at helpline@crohnsandcolitis.org.uk. Lines are open Monday to Friday, 9am to 5pm, (except English bank holidays).
If you are a parent of a child, there is information about Crohn’s disease and ulcerative colitis in children from CICRA at www.cicra.org.
If you have been diagnosed with bowel cancer, you can find out more information from the charity Bowel Cancer UK at www.bowelcanceruk.org.uk.
What to ask your doctor?
- How can I best self-manage my condition?
- Are there over the counter remedies which may be useful?
- How can I prevent my condition from returning?
- Do I need further investigations?
Discover more:


{kind=link}
Copyright © 2026 Guts UK. This leaflet was published by Guts UK in October 2025 and will be reviewed in October 2028. The leaflet was written by Guts UK and reviewed by experts in perianal disease and has been subject to both lay and professional review. All content in this leaflet is for information only. The information in this leaflet is not a substitute for professional medical care by a qualified doctor or other healthcare professional. We currently use AI translation tools on our website, which may not always provide perfect translations. Please check for further explanation with your doctor if the information is unclear. ALWAYS check with your doctor if you have any concerns about your health, medical condition or treatment. The publishers are not responsible or liable, directly or indirectly, for any form of damages whatsoever resulting from the use (or misuse) of information contained or implied in this leaflet. Please contact Guts UK if you believe any information in this leaflet is in error.