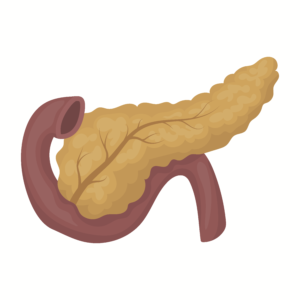
 The pancreas is a key organ required for the digestion process. It has two main roles: first is the production of pancreatic digestive enzymes (exocrine function) and the second is the production of insulin and other hormones for the regulation of blood glucose (endocrine function). Either, or both of these, are frequently affected by diseases such as pancreatic cancer, acute and chronic pancreatitis.
The pancreas is a key organ required for the digestion process. It has two main roles: first is the production of pancreatic digestive enzymes (exocrine function) and the second is the production of insulin and other hormones for the regulation of blood glucose (endocrine function). Either, or both of these, are frequently affected by diseases such as pancreatic cancer, acute and chronic pancreatitis.
I am part of a large dietetic department in a teaching hospital which is a national specialist centre for pancreatic surgery. I work closely within the upper Gastrointestinal, pancreatic, and general surgical mini team. Teamwork is key for all health professionals within healthcare. My day starts by liaising with my dietetic colleagues. We meet every morning in a “huddle” to discuss everyone’s case load including new referrals into the service, reviews, and ward discharges. The huddle ensures everyone has an appropriate case load in terms of numbers and complexity and is designed to ensure everyone feels supported.
Following the huddle I attend the specialist inpatient ward which is home to pancreatic surgical patients and acute pancreatitis patients. The most common surgical operation undertaken in our centre is the Pylorus Preserving Pancreaticoduodenectomy – which is quite a name so frequently (always) is abbreviated to a PPPD during verbal handovers of patient information between various members of the MDT (multidisciplinary team) including doctors, nurses, pharmacists, physiotherapists and others who are involved in the rehabilitation of patients after major surgery.
 A typical day would see me discussing ways of improving a patient’s nutritional status by helping manage their symptoms thus improving their ability to eat and absorb their food and drink.
A typical day would see me discussing ways of improving a patient’s nutritional status by helping manage their symptoms thus improving their ability to eat and absorb their food and drink.
During the initial assessment of a patient, a pancreatic dietitian will assess nutritional status which involves asking about a patient’s weight changes and appetite. Dietitians also consider and interpret relevant previous medical history, biochemistry, fluid balance and any complications after surgery that have occurred. As surgery takes several weeks to recover from, it is essential to maximise how well people eat during this time to help with wound healing and energy levels.
During a dietetic assessment, a pancreatic dietitian will be monitoring for signs as to whether the pancreatic resection has caused the patient to develop diabetes and pancreatic enzyme insufficiency. I work very closely with the diabetes specialist nurses and doctors regarding the management of diabetes and pancreatic enzyme insufficiency.
Once a week I attend the MDT (multi-disciplinary team) pancreatic surgical outpatient clinic. Within this clinic, I see patients who have been newly diagnosed with pancreatic cancer or returning to clinic after being discharged form hospital after having a pancreatic resection. It is always lovely to see patients as they are recovering and getting back to a more normal life.
A large proportion of my day is recording and documenting electronically my assessment, treatment plan and next review date. Dietetic records can be accessed by any member of the relevant teams and ensure a coordinated care plan is established.
This is the essence of my typical day, but every day is different. It may even include training a dietetic student and contributing to various meetings focused at development, team, MDT, time outs to name a few.

 ABOUT US:
ABOUT US:





