Microscopic Colitis
Download printable versionOverview
Microscopic colitis (MC) is an inflammatory bowel disease (IBD). Symptoms include watery diarrhoea, along with urgency and bowel control issues. People often have night-time symptoms, which can be unrelenting. People affected often need to find toilets when they leave home, to avoid accidents. In some cases, people are unable to leave the house at all due to the severity of their symptoms. Symptoms can be severe and lead to a substantial loss of quality of life.
Microscopic colitis can develop at any time. But it is more common in middle age. Most people are diagnosed between the ages of 50 and 70. But it can be diagnosed in all ages, including rarely in children. In people 65 years of age or over with diarrhoea, as many as 1 in 5 might have microscopic colitis. It also occurs more often in women and can occur earlier in people who smoke cigarettes. 1 in 2,000 people have microscopic colitis in the UK. But reported rates vary widely. Figures are likely to be an underestimate because it is often misdiagnosed or missed. This is because current stool and blood tests for other inflammatory bowel diseases do not pick up microscopic colitis.
Importantly, good medications to bring about remission exist for this condition. Remission means symptoms resolve or are much reduced. But it may not be identified as a diagnosis. So, Guts UK aims to raise awareness among the public and health professionals.
Causes
It is not yet clear what causes microscopic colitis. There are some risk factors, like having bile acid diarrhoea, and some medicines can cause it.
Medications linked to microscopic colitis include:
- Non-steroidal anti-inflammatory drugs (e.g. ibuprofen, aspirin)
- Protein pump inhibitors (e.g. lansoprazole)
- Statins (e.g. simvastatin)
- Some H2 antagonists (e.g. famotidine)
- Some diabetic meds (e.g. acarbose)
- Some antidepressants (e.g. sertraline)
- Some anticoagulants (e.g. ticlopidine)
- HRT (in high doses)
- Some anticonvulsants (e.g. carbamazepine)
Always discuss medications with your doctor. Do not stop taking any without their advice.
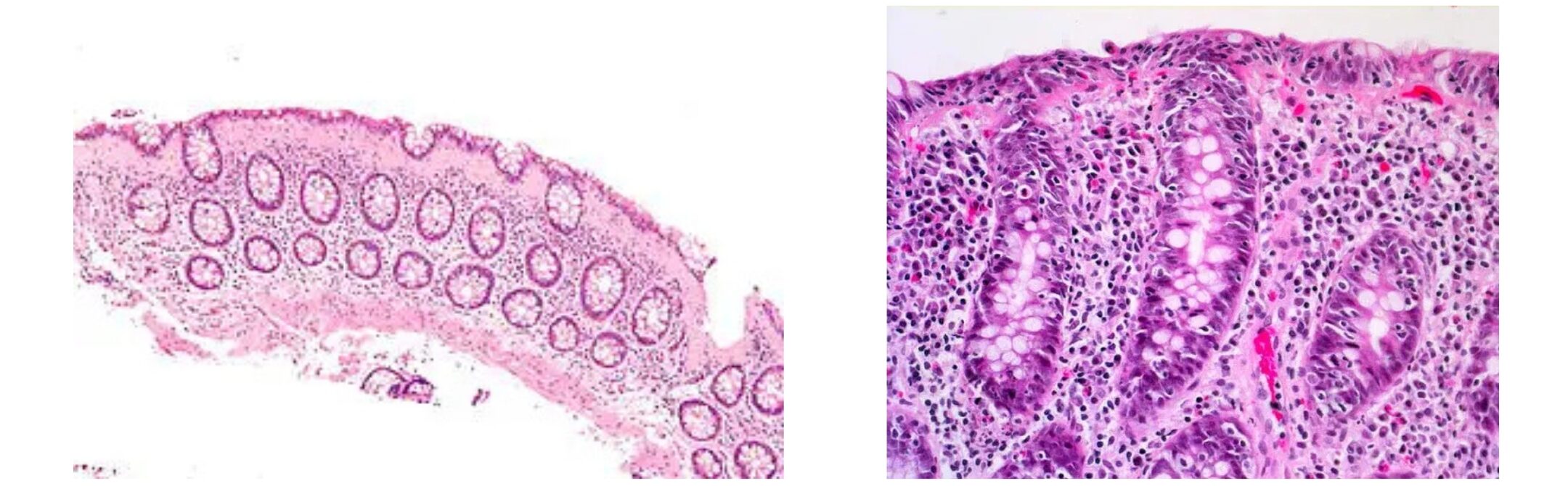
There are two types of microscopic colitis:
- Lymphocytic colitis. This is where there are more white blood cells (lymphocytes) in the lining of the bowel. White blood cells fight infection.
- Collagenous colitis. This is when the bowel lining has a thicker layer of collagen. Collagen is a protein that forms the connective tissue in the bowel wall.
The bowel lining looks different under a microscope depending on the type of microscopic colitis. But the symptoms and treatment are the same.
Symptoms
Symptoms of microscopic colitis include:
- Watery diarrhoea.
- Bowel incontinence episodes.
- Waking during the night to empty the bowels.
- Urgency to use the toilet.
- Frequent need to empty the bowels (can be many times in 24 hours).
- Abdominal pain.
- Unexplained weight loss.
- Bloating.
It’s important that people know of the symptoms of microscopic colitis so that those affected can discuss it with their doctor. This is true for both the undiagnosed and those unsure of their treatment. Considering more symptoms and signs, along with watery diarrhoea, may help diagnosis.

Microscopic colitis can occur with other autoimmune diseases. These include:
- Some thyroid problems
- Coeliac disease
- Rheumatoid arthritis
- Psoriasis
- Type 1 diabetes
A close blood relative might have an autoimmune disease, even if the autoimmune disease doesn’t affect them.
Diagnosis
This condition is thought to be under-diagnosed. So, people with these symptoms might have misdiagnosed microscopic colitis. It is often misdiagnosed as irritable bowel syndrome (IBS) or diverticular disease. Figures suggest 1 in 10 people with IBS with diarrhoea (IBS-D) may have microscopic colitis.
Unfortunately, they may have had symptoms for many years before diagnosis, when an effective treatment was available. This is partly due to low awareness among some health professionals. It is also due to how the condition appears. Unlike other inflammatory bowel diseases (IBD), like Crohn’s disease and ulcerative colitis, the bowel lining looks normal when viewed with a colonoscope (a flexible tube with a camera for examining the bowel). Also, unlike other IBD, the faecal calprotectin poo test cannot show signs of microscopic colitis.
The blood tests that are used to check for infection c-reactive protein (CRP) and erythrocyte settlement rate (ESR) also may miss microscopic colitis. The results of tests may be normal or only slightly raised. A normal result can falsely reassure people. Faecal calprotectin test or blood tests for infection do not rule out microscopic colitis.
Only a biopsy (a small tissue sample) from the large bowel wall can detect the inflammation. Multiple biopsies are recommended to be taken, and they should be taken from different areas of the large bowel including the left and right side. By taking more biopsies, it increases the likelihood of diagnosing microscopic colitis. A pathologist must then examine it under a microscope to find out the type of microscopic colitis.
People with microscopic colitis should be tested for coeliac disease as people can have both.
Treatment
Microscopic colitis is a lifelong condition but there are ways that can bring the disease into remission. The correct diagnosis and treatment can make a dramatic improvement to the person’s quality of life. Current data suggests a diagnosis of microscopic colitis does not increase the risk of bowel cancer. Some data suggests that, without treatment, some people need to stay in hospital during a flare of symptoms.
If the cause of the microscopic colitis is a medicine, your doctor may ask you to stop taking it. They could consider giving you other options instead. This can often result in symptom improvement. Do not stop taking any medication without your doctor’s advice.
Stop smoking if this applies to you. Stopping can be challenging, and people are usually more successful with help. Ask your GP about smoking cessation services in your area.
There is no evidence that diet can induce remission but if you suspect that food is affecting your symptoms talk to your doctor. Your doctor can arrange any testing for coeliac disease and referral to a dietitian if required. Please do not stop eating gluten (wheat barley and rye) as this needs to be consumed to identify coeliac disease, where it is present. Excluding gluten could result in a false negative result. Discuss it with your doctor if this is a problem. Whatever your results, include a good variety of foods in your diet within any restriction advised by your doctor or dietitian.

Microscopic colitis can be treated with gut-specific steroids (budesonide). This is usually the first choice of treatment. You may be asked to lower your dose gradually to find the lowest dose that treats symptoms. If your symptoms return tell your doctor.
If budesonide doesn’t work well or it is not tolerated, then other treatments can be considered. These treatments are often used for other inflammatory bowel diseases. For example:
Azathioprine or 6-mertcaptopurine. These medicines work by suppressing the immune system. The immune system is over-active in microscopic colitis.
Anti‐tumour necrosis factor (TNF) medicines adalimumab or infliximab. These medicines target the specific factor in the immune system that leads to inflammation1.
Vedolizumab is a type of biologic medicine and can be used to treat microscopic colitis. It is administered every 2 to 8 weeks by regular intravenous drip or injection under the skin. It is now available in a form that people can give it themselves rather than have it administered in hospital. Ask your consultant if you would benefit from these treatments.
Loperamide, an anti-diarrhoeal medication or cholestyramine, a treatment for bile acid diarrhoea, can sometimes be used in combination with budesonide as treatment.
Steroids, in particular budesonide, work for most. But some people may need more tests or other treatment. So, there are ongoing studies on other treatments, including drugs and by modifying the bugs found in the large bowel to establish what treatments are most effective.
If symptoms continue, your doctor should consider other diagnoses. For example, coeliac disease, lactose intolerance, and bile acid diarrhoea.
Support
What to ask your doctor?
- Are my symptoms due to microscopic colitis?
- Are my medicines causing my symptoms and are there any alternatives?
- Would I benefit from a colonoscopy and a biopsy of my large bowel?
- Do I need to be tested for other autoimmune conditions such as coeliac disease?
What other resources and organisations can help?
Microscopic colitis is a form of inflammatory bowel disease and you can find out more information from:
Crohn’s and Colitis UK (CCUK)
Crohn’s and Colitis UK are the leading charity working on Crohn’s disease and other inflammatory bowel diseases.
The British Society of Gastroenterology (BSG) has also produced a video on microscopic colitis, available to watch here.
Watch our microscopic colitis webinar on demand
Discover more about microscopic colitis and hear from healthcare professionals and people with lived experience of the condition:
Discover more:



Copyright © 2026 Guts UK. This leaflet was published by Guts UK in May 2025 and will be reviewed in May 2027. The leaflet was written by Guts UK and reviewed by experts in polyps and has been subject to both lay and professional review. All content in this leaflet is for information only. The information in this leaflet is not a substitute for professional medical care by a qualified doctor or other healthcare professional. We currently use AI translation tools on our website, which may not always provide perfect translations. Please check for further explanation with your doctor if the information is unclear. ALWAYS check with your doctor if you have any concerns about your health, medical condition or treatment. The publishers are not responsible or liable, directly or indirectly, for any form of damages whatsoever resulting from the use (or misuse) of information contained or implied in this leaflet. Please contact Guts UK if you believe any information in this leaflet is in error.