




Flushing away the poo taboo, together!
What is it that stops us from talking about our digestive health, or poo, as openly as we’d talk about having a cold, a headache or back pain? After all, our poo is an indication...
7th March 2024
16th May 2020
Guts UK is one of the many worldwide charities collaborating to raise awareness of Barrett’s oesophagus for the first ever World Barrett’s Day – 16th May 2020.
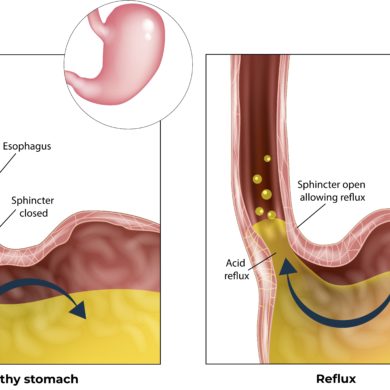
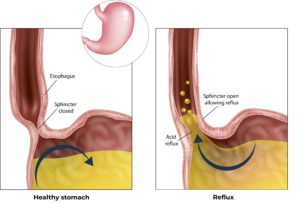 Around 10% of persistent heartburn sufferers who have longstanding reflux problems may develop a condition called Barrett’s oesophagus where the cells in the oesophagus start to change colour. Often (but not always) the lining of the oesophagus starts to resemble the lining of the stomach. The exact cause of Barrett’s is unknown, but its link to longstanding reflux is clear. Patients with Barrett’s are more likely to develop oesophageal cancer.
Around 10% of persistent heartburn sufferers who have longstanding reflux problems may develop a condition called Barrett’s oesophagus where the cells in the oesophagus start to change colour. Often (but not always) the lining of the oesophagus starts to resemble the lining of the stomach. The exact cause of Barrett’s is unknown, but its link to longstanding reflux is clear. Patients with Barrett’s are more likely to develop oesophageal cancer.

It is thought that there are many individuals in the UK with undiagnosed Barrett’s oesophagus. Diagnosing Barrett’s is important, as it’s vital that those with Barrett’s are monitored. Patients with Barrett’s oesophagus are at higher risk of developing oesophageal cancer, so diagnosis and regular monitoring of the Barrett’s is crucial.
 Guts UK & Olympus currently fund research fellow Dr Sara Jamel. Dr Jamel was awarded £210,000 for a 3-year project starting in 2019. Her innovative project will explore the use of breath-testing for pre-cancerous cell changes in patients with Barrett’s oesophagus. If successful, this breath test could save lives by diagnosing oesophageal cancer early, when it is far more treatable.
Guts UK & Olympus currently fund research fellow Dr Sara Jamel. Dr Jamel was awarded £210,000 for a 3-year project starting in 2019. Her innovative project will explore the use of breath-testing for pre-cancerous cell changes in patients with Barrett’s oesophagus. If successful, this breath test could save lives by diagnosing oesophageal cancer early, when it is far more treatable.
Read more about Dr Jamel’s research.
Only 12% of people survive oesophageal cancer for longer than 10 years, yet 59% of oesophageal cancer cases are preventable. Our research has the capacity to change these facts and save more lives.
Guts UK want to fund research that directly benefits people who are affected by digestive conditions conditions, as well as their families and carers. The best way to understand the needs and priorities of people who suffer with digestive disorders is to ask them. In 2016, in collaboration with other organisations, we did exactly that. We brought together patients and healthcare providers to identify their top ten priorities for research on Barrett’s Oesophagus, a disease that affects the gullet (oesophagus), as well as its cause: acid reflux (also known as gastro-oesophageal reflux disease).
|
1. |
How can we accurately identify the high-risk people from the general population to target Barrett’s Oesophagus screening? |
|
2. |
How can we achieve individual risk stratification of patients with Barrett’s Oesophagus in order to target surveillance more appropriately? |
|
3. |
Is there a more acceptable, cost effective and accurate test for surveillance and screening of Barrett’s Oesophagus in a primary care setting? |
|
4. |
Should Barrett’s surveillance and new patient clinics be conducted by a dedicated service? How would this compare to current standards of practice in the UK and what impact would this have on patients? (for example, pre- cancer diagnosis rates, patient education, quality of life and satisfaction) |
|
5. |
What is the long-term effectiveness of endoscopic treatment (RFA) for precancerous Barrett’s or early cancers? How does this effect the need for future endoscopic surveillance in these patients? Is there a role for other methods such as cryoablation or APC in these care pathways? |
|
6. |
Are there any long-term complications or risks with prolonged PPI use? Particularly their effects on bone density, salts in the blood (electrolytes), kidney function and cognitive impairment? |
|
7. |
How does a patients genetic makeup relate to their risk of disease progression at a cellular level (from Reflux – Barrett’s Oesophagus – Precancerous – Cancer)? Particularly in younger patient groups, those with a strong family history or those with disease recurrence after endoscopic treatment (ablation)? |
|
8. |
Are PPIs the only long term answer for treating reflux? What other treatment options are available for patients who are intolerant, unresponsive or unwilling to take PPIs? (for example, surgery, newer medications or minimally invasive techniques such as endostim and stretta) |
|
9. |
Is “blanket” surveillance of all Barrett’s Oesophagus beneficial to patients or cost effective in its current model? Are current surveillance intervals appropriate and when can surveillance be safely discontinued? |
|
10. |
Is there a role for anti-reflux surgery to prevent Barrett ‘s with no precancerous changes progressing or to prevent disease recurrence after endoscopic treatment for pre-cancer? |
 ABOUT US:
ABOUT US:Guts UK’s vision is of a world where digestive diseases are better understood, better treated and where everyone who lives with one gets the support they need. We fund life-saving research into diseases of the gut, liver and pancreas.
Champion our cause; help us fight digestive diseases and change the lives of millions of people in the UK by supporting our work today.
What is it that stops us from talking about our digestive health, or poo, as openly as we’d talk about having a cold, a headache or back pain? After all, our poo is an indication...
7th March 2024
We’re delighted to take our free ‘Science of Digestion’ event to Hull next month (Tuesday 14th May 2024!) This is your opportunity to learn all about the hidden world inside your guts and the latest...
22nd April 2024

Download printable version (337.3KB pdf) OVERVIEW You might have noticed supply issues with pancreatic enzyme replacement therapy (PERT), sometimes also called pancreatin. This situation has progressed. It has now caused some people who need PERT...
16th April 2024

By submitting this form, you are consenting to Guts UK contacting you by email as detailed above. To make any changes to your preferences you can email us on info@gutscharity.org.uk or by calling us on 020 7486 0341. Your details are safe with us. Please read our Privacy Policy for more details.