Polyps in the bowel
Download printable versionOverview
This factsheet is about polyps in the large bowel.
A polyp is a fleshy growth on the inside of the large bowel. Some people may develop just a single polyp, while others may develop many.
Polyps are very common, especially in the Western world, and are a little more commonly found in men than women. They are unusual below the age of 40 and seem to occur most often in people over the age of 60. They affect one in four people over the age of 50 years.
What does a polyp look like?
When a doctor or nurse looks inside the large bowel with a special camera called
a colonoscope, they might see polyps. Polyps can look very different. Some polyps
have a stalk (which can look like a mushroom growing from the lining of the bowel) (Fig.1) or it can be much flatter and even have quite a broad base. (Fig.2)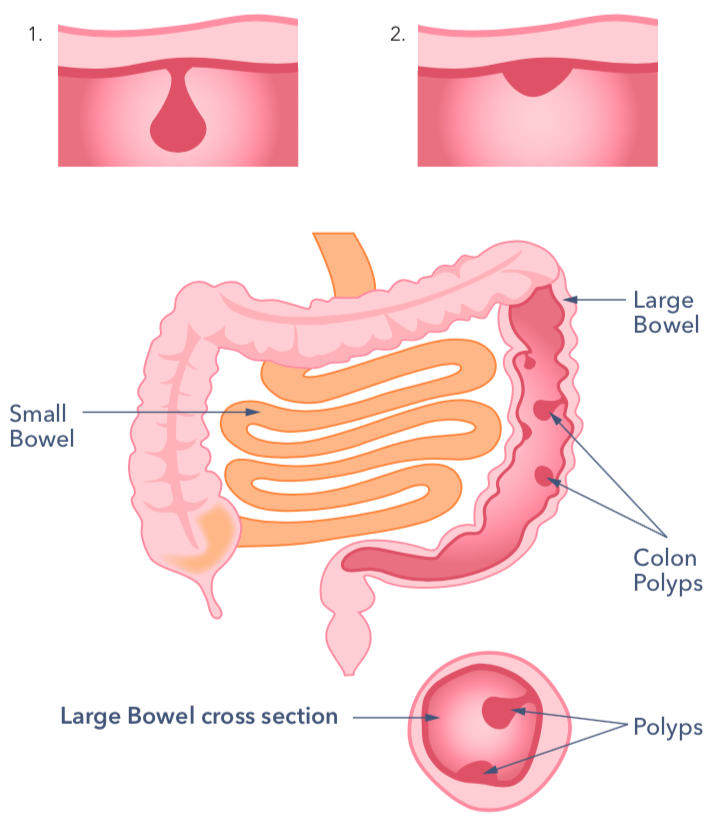
Polyps are usually benign (harmless – not containing cancer). But it’s important
they are removed because some of them may eventually develop cancer inside
them. Most experts now believe that most bowel cancers develop from polyps.
Doctors are most worried about detecting and treating a type of polyp called an
adenoma polyp. This is because adenomas are the type of polyps that are most
likely to become cancerous in the future. It is thought that if left alone around 1
in 10 adenomas would develop into cancer.
Causes
What causes the development of polyps in the bowel?

The lining of the bowel, like other organ linings, constantly renews itself throughout our lives. There are many millions of tiny cells in the lining, which grow, serve their purpose and die. New cells then take their place. Each of these millions of cells contains genes, which give instructions to the cell on how to behave and grow. If genes become faulty, this can cause the cells to grow quicker. Cells that are faster growing eventually produce a small bump on the bowel surface that we call a polyp.
Some polyps remain very small (less than one centimetre) while others continue
to enlarge up to several centimetres.
Most polyps remain harmless (non-cancerous), but it is thought that most cancers of the bowel begin as benign polyps. So, by removing benign polyps we can help to prevent the development of the rare ones that may become cancer
Can polyps be inherited?
Most people with polyps and cancers in the bowel do not have a genetic condition in their family. However up to 1 in 10 people who have polyps may have them because they are inherited (runs in families). When several members of the same family have had polyps or bowel cancer there is an increased risk. The risk is higher if they have developed polyps or bowel cancer at a young age. Some of the conditions which are inherited and can cause bowel cancer are:
- Lynch Syndrome
- Peutz Jeghers Syndrome (PJS)
- Juvenile Polyposis Syndrome (JPS_
- Multiple endocrine neoplasia (MEN) type 1 and 2
- Familial adenomatous polyposis
Tell your GP if you have a family history of the above conditions or if more than one person in your family has had bowel cancer.
Diagnosis
How are polyps in the bowel diagnosed?
Bleeding from the back passage (rectal bleeding) is a symptom of both benign and malignant polyps,as well as other potentially serious conditions. Investigations will be carried out to figure out whether any of these conditions are the cause of the bleeding.
Faecal Immunochemical test (FIT):

FIT home testing kits can pick up hidden blood in poo that is not visible to the naked eye. The results of this test can help doctors decide whether someone needs to see a specialist or have more tests done. FIT is not a direct test for polyps, but it can show that polyps might be present in the large bowel, leading to a referral from your doctor for a colonoscopy (see below). You might be asked to do a FIT test as part of the UK bowel cancer screening programme.
Even if you have done a FIT as part of the screening programme, it is still also
important to look for any change in bowel habits. If you have any of the following
symptoms then seek advice from your GP:
- An ongoing change in your bowel habit
- Bleeding from the bottom without any obvious reason
- Abdominal pain
- A lump in your belly (abdomen)
Colonoscopy:
This is where a tube, linked to a highly magnified video system is passed via the
anus, into the large bowel. Plus, where possible, the nearest part of the small
bowel. A colonoscopy gives a very accurate picture of the lining of the bowel. It
also allows the doctor, or nurse endoscopist, to check for polyps. The endoscopist
can remove polyps during the procedure. Sometimes a shorter camera called a
sigmoidoscopy is used. The sigmoidoscopy only allows inspection of the lower
bowel. If it reveals a polyp, a full colonoscopy may be needed to check that there
are no more polyps further into the large bowel. You can choose to have sedation
to minimise any feelings of discomfort or anxiety.
CT Pneumocolon Scans:
This involves air being introduced into the bowel by a small tube. The air improves the views of the bowel while the scanning is happening.
Except for FIT all of the above will require the bowel to be as clear as possible before the procedure. An empty bowel is needed so that any polyps can be seen. A special diet is followed for a short period, and laxatives (medicines to make you poo) are taken at home the day before the procedure. Although this is not pleasant, the laxatives are taken in the right amount to clear the bowel. This will cause diarrhoea therefore and it is a good idea to stay near a toilet

We encourage everyone who is eligible to take part in the FIT test screening programme.
In England all men and women aged 60 to 74, who are registered with a GP are automatically sent a bowel screening test every 2 years. In 2021 this will include people aged 56. The age range is planned to be expanded to age 50 over the next 4 years.
In Scotland screening starts at aged 50 to 74. In Wales the age range is 58 to 74. In Ireland the age range is 60 to 69.
If you live in England and are over 75 years of age you can ask for a kit every 2 years. You can request one by phoning 0800 707 6060.
Another time you might be asked to do a FIT test is if you go to your doctor with bowel symptoms.
If the test is positive your doctor will discuss this with you and might refer you for a colonoscopy – as long as this is safe, and you don’t mind having it.
The FIT test might be unpleasant, but it is a small job to perform that has real and potentially life-saving benefits.
Symptoms
How can polyps in the large bowel affect you?
Usually polyps do not cause symptoms and most people will never know if they have them. They are usually found when people have a colonoscopy for another reason.
Symptoms
Polyps are often discovered at colonoscopy as part of an investigation into bowel changes or symptoms. Usually, the polyps are not the cause of those symptoms. Occasionally they can cause bleeding from the back passage. Or may produce an excess of mucus or slime, which can be noticed on motions when opening the bowel. Very occasionally a polyp can grow so large as to cause a blockage of the bowel but, unless this occurs, polyps do not cause pain.
Will polyps in the bowel affect me over time?

Polyps rarely cause day to day problems. However, the main concern is that they may become harmful and cause cancer in the future. Most polyps can be taken off at the time of your colonoscopy, however in some cases, such as for very large polyps, another procedure may be required. If polyps are found and removed, they are looked at under a microscope. If cancer changes are found within the polyp, then further tests, such as scans, will be needed at that time.
If the polyps do not contain cancer, you will be told either that nothing else is needed or that you should have another colonoscopy in a few years to keep an eye on things. This depends on the number of polyps found and whether they were low or high risk types. The British Society of Gastroenterology (BSG) have developed some guidance on who needs surveillance, and the guidance is available from the BSG website. If you need a printed copy, please contact Guts UK.
You should still complete the FIT screening test every 2 years (if you are eligible) as things can change. If you have a family history of either polyps or bowel cancer, then your doctor may also recommend that you have a regular colonoscopy.
It should be remembered that the risk of colonoscopy is small, but in some people even though small it might outweigh the benefits of screening. Discuss this with your doctor.
Diet
 You do not need a special diet and can eat normally. However, a healthy diet, which includes a wide variety of foods and plenty of fruit and vegetables, is good for your general health and to produce good bowel movements. Aim to have regular fruit and vegetables (with meals as well as snacks) and to drink at least two litres (8-10 cups) of fluid every day.
You do not need a special diet and can eat normally. However, a healthy diet, which includes a wide variety of foods and plenty of fruit and vegetables, is good for your general health and to produce good bowel movements. Aim to have regular fruit and vegetables (with meals as well as snacks) and to drink at least two litres (8-10 cups) of fluid every day.
Please see Guts UK’s Healthy Eating & The Digestive System information here.
Treatment
What treatment is available?
There are a variety of different techniques to remove polyps. Most consist of passing a wire through the colonoscope and looping wire around the polyp – like a lasso – to remove it. This procedure is quite painless and only one examination is usually needed to clear the bowel of polyps. Every once in a while, there may be too many polyps for all of them to be removed safely at once. In these cases, the procedure may need to be repeated.
Removal of a polyp using a colonoscope and a looping wire:
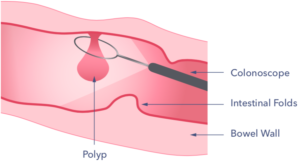
Once they have been removed, the polyps are sucked up through the colonoscope if possible. They can then be sent to the laboratory to be looked at under a microscope. This will show whether the polyp has been completely removed, whether there are any pre-cancerous changes and of course, to be sure that cancer has not already developed.
Support
What to ask your doctor?
- What type of polyp do I have, is it benign or malignant?
- How often should I have a follow up colonoscopy?
- Has my family history been noted and taken into account?
- What other follow up do I need?
Where can I get more information?
The British Society of Gastroenterology (the professional body for gastroenterologists) produce guidelines with a summary for people with polyps and their families and carers and it can be found on the British Society of Gastroenterology website.
You can find out more about FIT testing here.
 How can I be involved in research?
How can I be involved in research?
Guts UK are proud to be funding research by Professor Colin Rees, COLO-COHORT (Colorectal Cancer Cohort Study) which aims to identify and build a more detailed screening programme for those who are at increased risk of developing bowel cancer. Bowel cancer, when identified early, is one of the more preventable cancers. This Guts UK-funded research has the capacity to save lives, by developing a robust screening programme for the UK and bowel cancer. Read more here.
It’s time the UK got to grips with guts.
If this information helped you, please donate to Guts UK charity today. With your support, we can continue writing and sharing information for those who need it most. Your donation will also fund life-saving research and raise much-needed awareness of digestive diseases and symptoms. Thank you for helping the UK get to grips with guts.



