Dr James Evans (Barrett’s Oesophagus)
2014 Derek Butler Fellow
Institution: Queen Mary University of London
Title: Investigating the clonal origins and dysplasia risk in Barrett’s oesophagus
Project Start Date: 6 October 2014
Completion Date: 5 October 2017
Summary:
There has been a large increase in the number of patients with cancer of the gullet in the UK over the last few decades. The major risk factor is a precancerous disease called Barrett’s oesophagus which is characterised by a microscopic change in the lining of the gullet from a normal simple cell layer to one that is thought to resemble the more complex organisation of the intestine. Barrett’s is common and cancer risk is low, but the large number of patients means cancer is a significant concern and as such patients are routinely examined. This is expensive and is not making a significant impact on the number of overall gullet cancer cases. We therefore need to understand how Barrett’s lesions form and evaluate when they are most likely to develop cancer.
We believe that Barrett’s does not in fact resemble the intestine but rather the stomach. Evidence from our laboratory demonstrates this and we hypothesise that Barrett’s originates from the stomach. Work comparing stem cells and the cells they produce in Barrett’s with those of the stomach will reveal their relationship. We will use novel technologies to read the DNA (the blue print of the cell) from mitochondria (the cell’s battery). Mutations in this DNA are common and we can trace which cells possess which mutation. This permits us to work back in time and detect the origins of each cell.
Furthermore, there are no validated means to predict the changes that lead to advanced precancerous Barrett’s. We propose that mutations acquired in mitochondria build up over time, and may reflect cancer risk and will follow patients over time to test this hypothesis and provide a better means to assess cancer risk and potentially decrease cumbersome endoscopic investigations.
I have set up specific collaborations with 3 pathologists;
Dr Marnix Jansen, Academic Medical Centre, Amsterdam. Dr Jansen is a pathologist who specialises in early cancer development. He is willing to provide frozen biopsies from patients who are routinely endoscoped with Barrett’s.
Professor Marco Novelli, Dept Histopathology, University College London Hospitals. Prof Novelli is a pathologist with a proven track record of investigating relationships between cells in pre-cancerous disease. He has kindly agreed to provide snap frozen tissue from patient who have had surgery to remove their gullet because of cancer.
Dr Manuel Ropdriguez-Justo, Dept Histopathology, University College London Hospitals. Dr Rodriguez-Justo is an expert gastrointestinal pathologist that has shown my host laboratory a great deal of support in providing fresh frozen specimens and assisting in obtaining consent from patients undergoing surgery.
The project has 3 main studies/hypotheses to be investigated:
Hypothesis 1 will use frozen gastrointestinal tissue taken from surgical resection/biopsies to compare single cells in Barrett’s glands and then whole glands between a small number of patients. It is difficult to predict how many patients will be required, however similar investigations in other organs has shown that between 5 and 15 patients will be required. This tissue has already been obtained. Next generation DNA sequencing and analysis of this data is expected to be complete within 12 months.
Hypothesis 2 will require samples from no more than 10 patients. Different sites from each patient’s gullet and stomach will be compared to look for different mutations. DNA sequencing will be performed on these samples and data production and analysis is again estimated at 12 months.
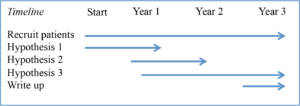
Hypothesis 3 will require samples over time from at least 25 patients. This will be analysed to determine mutations in cells over time. Recruitment for these patient and obtaining samples will begin on starting the project in year 1 and continue in to the third and final year.
Interim Reports will be submitted annually showing data for each hypothesis each year respectively. Final report is to be prepared and completed in the final 6 months of year 3 and completed by 01/08/2017.
My proposed timeline of experiments and thesis completion is below:
Although this project is unlikely to have immediate clinical benefits it will increase our knowledge of how Barrett’s develops in to oesophageal cancer. We hope this will allow the wider scientific community to predict which patients are most likely to develop changes in cells within Barrett’s oesophagus that lead to cancer thus allowing more efficient risk stratification of patients and save on expensive investigations. I intend to submit my work for presentation at local, national and international meetings. I intend to use these meetings to allow the development of new contacts and collaboration, disseminating my research through the wider scientific community. By establishing how Barrett’s develops we hope to enable universal guidelines to be published.
This ambition has been nurtured over the course of the last three years after having been exposed to a portfolio of clinical and pre-clinical trials during my specialist training in gastroenterology. I have experience as an investigator in a study evaluating post oesophagectomy outcomes inpatient with oesophageal cancer. I have also seen the difficulties in providing extensive endoscopic screening for Barrett’s. This repeated testing is currently expensive and inefficient and requires further research to allow more targeted approach to screening for this condition. These experiences allowed me to develop my academic and research interests in upper GI malignancy including the role of Barrett’s in oesophageal cancer progression.
This project will improve my understanding of the fundamental processes underpinning the development of normal gullet to the pre-cancerous condition of Barrett’s. In my future practice I believe that being an expert in the field of Barrett’s will improve my approach to patients not just with this condition but a range of digestive diseases. It will improve my assessment at endoscopy at the inpatient and outpatient care setting. This project will also make me more analytical in my approach to patient care and treatment generally.
My career ambition is to become an academic clinical scientist with a strong interest in translational science that drives collaborative multicentre clinical trials within an academic institute. This ambition has been realised over the course of the last three years during my specialist training in gastroenterology. I am interested in continuing research in conditions affecting the gullet and stomach with a particular focus on developing better understanding of the mechanisms that underlie cancer forming in these sites. I wholeheartedly believe that understanding the fundamental processes within disease leads to better clinical trials and vice versa. I would like to continue further research in to trials for novel strategies to better predict the risk of cancer in Barrett’s patients in the future and to play a leading role in the development of treatments to maintain the eradication of Barrett’s.