Pancreatic Exocrine Insufficiency (PEI) and Pancreatic Enzyme Replacement Therapy (PERT)
Download printable versionOverview
What is Pancreatic Exocrine Insufficiency?
Any disease that affects pancreatic tissue can cause PEI. The most common causes in the UK are cystic fibrosis, acute and chronic pancreatitis and pancreatic cancer. Eight out of ten individuals with chronic pancreatitis will eventually develop PEI. PEI may also occur after pancreas surgery. It is possible to have a good quality of life with PEI.
The digestive system’s organ, the pancreas, has two main functions. The first
function of the pancreas is to make digestive enzymes which help in breaking
down food into its’ smaller parts. Food in its simpler form can then be absorbed
(taken in) through the wall of the small bowel and into the blood stream. The
secretion of pancreatic enzymes into the small bowel is referred to as its exocrine
function. The term “pancreatic exocrine insufficiency” (PEI) refers to the inability
to manufacture adequate enzymes. The pancreas’ second function is to create
insulin after the body has digested the smaller dietary components. Insulin
(a hormone) transports glucose from the bloodstream to the body’s cells, where
it is converted into energy. This is called the endocrine function. This information concentrates on the enzyme (exocrine) function of the pancreas.
Causes
What causes PEI?
Any disease that affects pancreatic tissue can cause PEI. The most common causes in the UK are cystic fibrosis, acute and chronic pancreatitis and pancreatic cancer. Depending on how severe the attack is, people who have acute pancreatitis with necrosis (pancreatic tissue death) could require PEI support.
PEI is common in chronic pancreatitis. Eight out of ten individuals with chronic pancreatitis will eventually develop PEI. PEI may also occur after pancreas surgery.
Occasionally, upper digestive tract surgery can result in PEI. Total gastrectomy
surgery for stomach cancer is one example, and up to 2 out of every 10 people
who have bariatric surgery for weight loss may have PEI.
Additionally, PEI could happen in 1 in 10, up to 1 in 2 people with type 1 diabetes
and 1 in 20, up to 1 in 2 people with type 2 diabetes. Diabetes develops when
sugar (glucose) from meals, which is ordinarily used as energy after digestion,
cannot enter body cells.
There are rarer causes of PEI which include Shwachman–Diamond Syndrome,
Johanson–Blizzard Syndrome, Pancreatic Hemochromatosis, as well as uncommon genetic metabolic errors such as Trypsinogen or Enteropeptidase Deficiency.
As people get older, there are more people diagnosed with PEI.
Pancreas and digestion
What is the role of the pancreas?
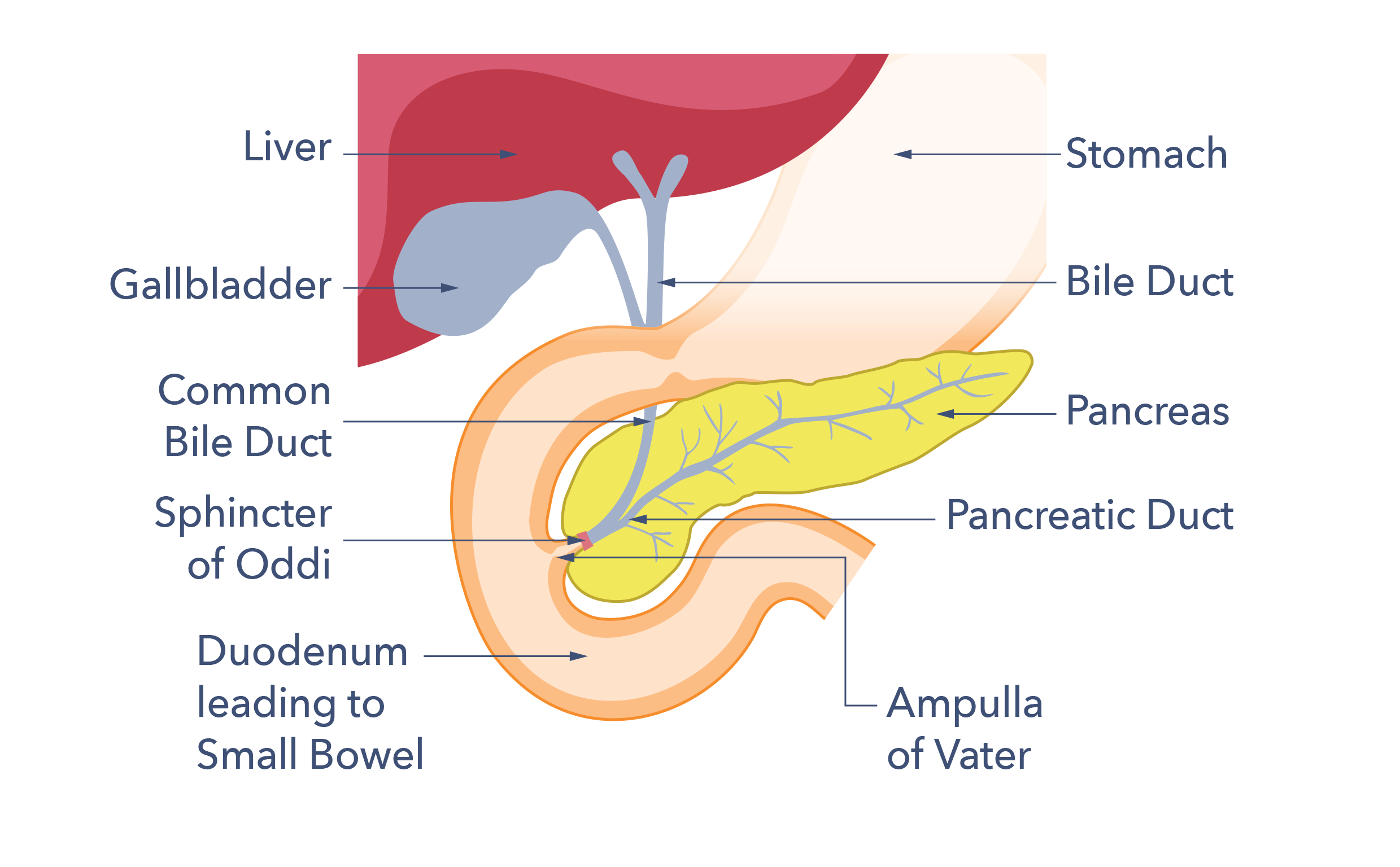
The pancreas gland is an essential part of the digestive and hormone systems of the body. It lies in the upper half of the abdomen behind the stomach and in front of the spine. It is salmon pink in colour, about 22cm (9 inches) long and about as thick as your wrist at its widest part. It makes both digestive enzymes and hormones.
To understand PEI, it may be helpful to learn more about the role of the pancreas in digestion. The foods we eat are made up of many different parts. Three of these are fats, proteins and carbohydrates. Energy for the body comes from both fats and carbohydrates. The building blocks for tissue growth and healing are provided by proteins. When there is a shortage of available carbohydrates, protein can occasionally be used to supply energy. The pancreas has a very important role in the digestion of all three.
Most dietary fat, protein and starchy carbohydrate molecules have complex structures. These structures are too big to be absorbed for use by body cells. Some of the carbohydrates in our food, such as sucrose (table sugar) or lactose (milk sugar), have much simpler structures. Even those still need to be broken down before they can be absorbed through the gut wall into the body. Another way of thinking about absorption is that the tiny food parts are soaked up into the body through the gut wall, a bit like a sponge.
The pancreas makes specialised chemicals called pancreatic enzymes that break down fat, protein and some carbohydrates into their smaller parts. One of the enzymes that perform this role is called amylase. Amylase breaks down the starchy carbohydrates found in foods such as bread, rice, pasta, potatoes and breakfast cereals. The fats in food are broken down into smaller parts called fatty acids and glycerol. The pancreatic enzyme responsible for this job is called lipase. Proteins are digested by pancreatic enzymes called proteases, which break them down into smaller molecules, known as peptides and amino acids.
In summary, pancreatic enzymes help convert:
- Starchy carbohydrates to glucose.
- Proteins to peptides and amino acids.
- Fats to fatty acids and glycerol.
This breaking down of food into smaller parts releases the nutrients the body needs to function and thrive. Food starts to be broken down in the mouth, with chewing and by mixing with saliva. Food is then swallowed and pushed through the gullet by muscular waves into the stomach. Stomach acid and the stomach’s churning motion also break up and mix food. The stomach eventually pushes its contents into the duodenum, the first part of the small bowel. The pancreas, which sits behind the stomach, contains a thin tube (the pancreatic duct). This tube runs through the pancreas to the top of the small bowel. The pancreas secretes pancreatic juice through this duct into the top of the small bowel to help enable digestion. Pancreatic juice contains pancreatic enzymes, as well as bicarbonate (a chemical), which neutralises the acid from the stomach.
How does PEI affect digestion?
In a damaged pancreas either not enough enzymes are produced, or the pancreatic duct is blocked, sometimes both happen. If not enough enzymes reach the top of the small bowel, the nutrients in food will not be digested well. They will continue to travel along the small bowel. When they reach the large bowel, the nutrients can produce unpleasant symptoms such as fatty diarrhoea, the medical term is steatorrhoea. The gut bacteria use the undigested nutrients for energy, and this causes belly (abdominal) pain, wind and bloating. The rest of the undigested food ends up being expelled from the body as poo. This process, where nutrients are not absorbed, is known as malabsorption. It’s important to note that a healthy pancreas has a large reserve capacity to produce enzymes and bicarbonate. PEI therefore happens slowly over time or after prolonged or severe damage (or if the duct is blocked).
Fat malabsorption tends to be the most visible problem in PEI for two reasons. Firstly, the mouth, stomach and small intestine also produce digestive enzymes. These may manage to break down proteins and carbohydrates enough to make up for a poorly working pancreas, at least at the start. The digestion of fat, on the other hand, is more reliant on pancreatic lipase production. This means that fat malabsorption tends to be an earlier and/or bigger problem in PEI. The second reason is that fat-malabsorption produces more obvious changes in bowel function than protein-malabsorption, making protein-malabsorption more difficult to diagnose. The diagnosis might be missed if there is not enough fat in the diet to cause the symptoms of fat malabsorption. However, weight loss, muscle wasting, and other symptoms of malnutrition can still occur. Low-fat diets only hide the symptoms of PEI and do not treat the real problem, therefore low-fat diets should not be used. One exception is when a person develops pancreatitis due to a hereditary disorder where there is too much fat in the bloodstream (Familial Chylomicronaemia Syndrome). A low-fat diet may be suggested for those with this rare diagnosis, and they should be referred to a dietitian for care.
What other roles does the pancreas have?
Endocrine function
The other role of the pancreas is called its endocrine function. Endocrine function controls how well sugar is taken into body cells. Endocrine function also requires the use of different specialised chemicals, such as the hormones insulin and glucagon. These hormones are secreted directly into the blood stream. Insulin prevents high blood sugar and glucagon prevents low blood sugar. They work together to keep blood sugar within a healthy range.
Different cells in the pancreas are responsible for its exocrine and endocrine functions. The bulk of the pancreas is dedicated to producing enzymes for digestion. The cells responsible for producing digestive enzymes are called acinar cells. Those that produce insulin and other hormones are in the pancreatic islets (or islets of Langerhans). These islets are distributed throughout the pancreas. This means that in addition to causing PEI, damage to the pancreas can also lead to problems with insulin and glucagon production. This causes a special form of diabetes called pancreatogenic (type 3C) diabetes. People with this form of diabetes can often experience difficulties managing their blood sugar levels. This is because both the chemicals insulin and glucagon, which are needed to manage high and low blood sugar well, are not produced in enough quantities by a damaged pancreas.
Symptoms
What are the signs and symptoms of PEI?
PEI can take time to develop and at first the symptoms might be mild. Symptoms can include:
- Belly discomfort or pain.
- Bloating.
- Wind.
- Fatty stools.
- Weight loss.
- Steatorrhoea (fatty poo) can look bulky, oily, pale orange/yellow, be foul-smelling and runny.
- Poo can also float and be difficult to flush away and may stain the toilet bowl.
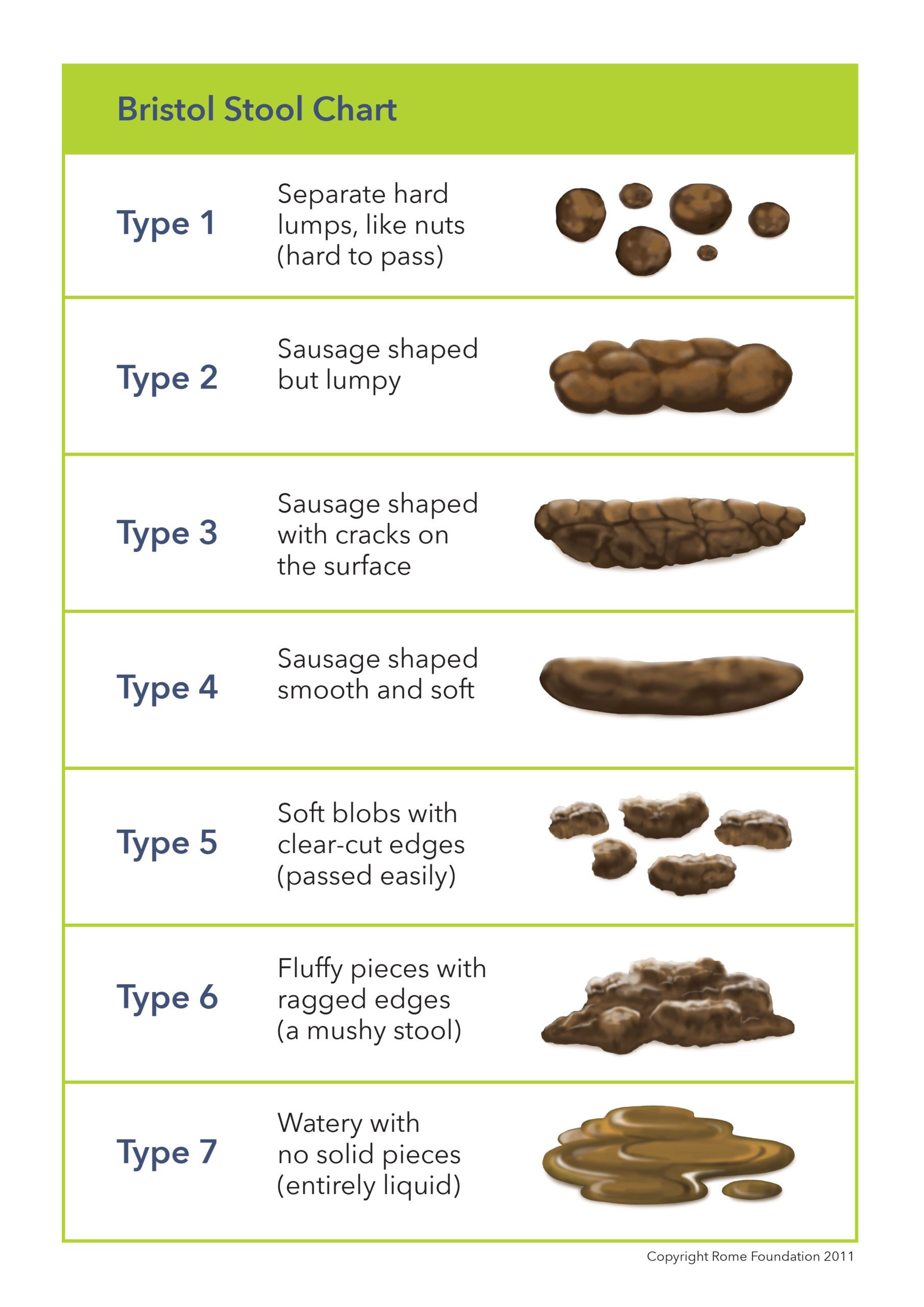
See the chart here. Type 6 to type 7 is defined as runny poo (diarrhoea).
Fat-soluble vitamins (vitamins A, D, and K) are found in foods containing fat. So fat malabsorption might lead to deficiencies in these nutrients over time. Low levels of these vitamins can give the following symptoms:
- Bone problems – osteoporosis.
- Bruising.
- Poor wound healing.
- Increased infections.
- Sight problems (particularly in the dark).
- Neurological (nerve) symptoms.
- Muscle weakness.
- Fatigue.
Some medicines causing constipation, such as codeine and other morphine-based medicines can mask the diarrhoea symptoms of PEI. Symptoms of weight loss and belly discomfort or pain, bloating and flatulence might still happen. Belly pain can also be a side effect of these pain killers.
How is PEI diagnosed?
The diagnosis of PEI is a skilled clinical procedure. The first stage is to ask about symptoms. This is then followed by an examination to look for signs of weight loss or malnutrition. If PEI is suspected tests will then be suggested. Tests will look at the structure of the pancreas (usually by an ultrasound, CT or MRI scan) and how well it is working, by a poo test.
The structural tests are called “imaging techniques” or “scans”. Ultrasound, CT and MRI scans all aim to look at the pancreas for evidence of damage to its tissue and its ducts. The tests highlight different features. More than one type of scan may be needed to build up a picture of the damage that has occurred. Magnetic Resonance Cholangio-Pancreatography (MRCP) is a special programme of the MR scanner which specifically views the ducts of the liver and pancreas. Ultrasound is usually performed by rubbing a probe over the abdomen. However, an internal ultrasound (Endoscopic Ultrasound, EUS) may give more detailed information in situations where a diagnosis is unclear. EUS is usually only available in the NHS in specialist centres.
The method used most in the UK to test the function of the pancreas measures the levels of pancreatic enzymes in poo. During normal digestion some of the enzymes secreted by the pancreas end up in poo. In PEI the lower levels of enzymes secreted into the duodenum means lower levels reach the poo. Measuring levels of pancreatic enzymes in the poo can give an indication of the levels produced by the pancreas. The most reliable enzyme to measure is a protease called elastase-1. Elastase-1 is not broken down as it travels through the gut and it concentrates in the poo. This test is called the faecal elastase-1 test (or FE-1). The levels of elastase-1 found in the poo can indicate whether pancreatic function is normal or how severe the PEI is. It is relatively convenient to test faecal elastase in poo as it does not require blood tests or invasive examinations. However, the test can fail to pick up cases of mild to moderate PEI. It can also sometimes give false positive results in other causes of diarrhoea.

There are other tests that measure, directly or indirectly, the function of the pancreas. These tests are not usually carried out in routine clinical practice and are not routinely available in the UK.
Sometimes the history, examination, scans and faecal elastase test agree, in which case the diagnosis is clear. Sometimes however, there is a disagreement between the different tests, or between the tests and the history. When that happens, further tests, for example an endoscopic ultrasound or tests for other digestive diseases may be necessary if there is no clear evidence of pancreatic disease. An experienced clinician will weigh up all these factors to arrive at a diagnosis and explain any other testing that might be needed.
Treatment
How is PEI managed and what is the role of Pancreatic Enzyme Replacement Therapy (PERT)?
Pancreatic enzymes are taken by mouth to compensate for the low levels produced by the pancreas in PEI. This is known as Pancreatic Enzyme Replacement Therapy (PERT), and it is the standard treatment for PEI. When taken properly PERT can improve fat, protein and carbohydrate absorption. PERT also reduces symptoms of fatty stools, wind and belly pain, increases body weight, and improves nutritional status and quality of life.
People with PEI take capsules containing pancreatic enzymes (lipase, amylase and proteases) with food. The capsules come in varying strengths; the dose can then be adjusted to suit the different requirements of people with PEI. They are taken with meals, snacks and milky drinks and release the enzymes in the top of the small bowel. This allows the food to be digested. PERT should be a part of a nutrition plan developed and managed by a specialist dietitian, who is a vital team member.
There are four different types of enzyme medicine available:
- Creon®
- Pancrease®
- Nutrizym®
- Pancrex®
They are available in either capsule or powder form.
Religious and ethical:
The enzymes are extracted from animal sources (pork) as being the closest in function to human pancreatic enzymes. Unfortunately, there is no vegetarian/vegan alternative currently available. If you have religious reasons to avoid pork products there are dispensations for medicines and medical conditions where they are essential for health and no suitable alternative is available. As there are no alternatives, the use is deemed acceptable by the Chief rabbi and most Muslim groups. Discuss this with your religious leader for support.
Alternative enzymes:
People with PEI should avoid seeking advice from other non-registered ‘nutritional therapists’. They have variable training and may give poor or dangerous advice. The British Dietetic Association can provide more information on the differences between a dietitian, a nutritionist, and other roles. The digestive enzymes that are promoted by health food shops and nutritional therapists contain tiny amounts of enzymes. Even though they are often marketed as vegan or vegetarian, unfortunately they are not likely to be effective. The only effective enzymes are those prescribed by a doctor, a nurse or a prescribing dietitian.
The only effective enzymes are those prescribed by a doctor, a nurse or a prescribing dietitian.
PERT & ongoing symptoms:
Often people with PEI taking PERT have a poor appetite. Eating smaller meals more often can help. If a person with PEI’s weight is stable and they are eating normally, there should be no need to change their meal pattern. It is important to ensure that the PERT dose is adequate and spread out throughout larger meals. There is no need to restrict fat routinely.
Occasionally people with pancreatic conditions can develop difficulty tolerating fat. If this is the case the PERT dose should be reviewed and possibly increased. If this does not help symptoms, other conditions should be investigated (such as bile acid diarrhoea, small bowel bacterial overgrowth and coeliac disease). Some people also need vitamin and mineral supplements, and this can be discussed with the dietitian. So don’t alter your diet to manage your symptoms. Instead, request a review of your digestive enzyme medicine from your doctor if you are having problems.
How to take PERT:
Many people with PEI are prescribed a standard ‘take two capsules three times a day with food’. This recommendation does not account for the size of the meal or cater for snacks or nutritious fluids such as milky coffee or hot chocolate. Successful PERT therapy relies on varying the number and/or strength of capsules taken according to the size and fat content of the meal. People with PEI may also be advised to take a part of their dose at the start, halfway through and at the end of the meal. As the individual’s dose of PERT varies, a starting dose should always be reviewed to check it is adequate for your digestive needs. PERT works directly on food, so it is important the capsules are in the stomach at the same time as food. Taking PERT on an empty stomach will not be effective.
Some meals take longer to eat (dining out in a restaurant, for instance) and ensuring that PERT is taken with each course will help the capsules mix with the food more effectively. Heat also damages the enzymes so do avoid leaving the capsules in direct sunlight, near radiators or in trouser pockets. Establishing successful PERT therapy requires a partnership between the person with PEI and their dietitian.
PERT & PPIs:
PERT is often prescribed with a proton pump inhibitor (PPI) medicine – examples are omeprazole, lansoprazole and esomeprazole, (there are several options). These medicines lessen the stomach’s ability to produce acid. In PEI the top of the small bowel may be more acidic than it should be. This is due to a decrease in the pancreas’ production of bicarbonate, which balances stomach acid. In an acidic environment, pancreatic enzymes cannot work.
As a result, the coating on PERT capsules prevents the enzymes from being activated in an acidic environment. The capsules won’t activate their enzymes at the proper time or location if the top of the small intestine is excessively acidic. They won’t function properly. The PPI medicine lessens the quantity of acid from the stomach reaching the small bowel and improves the action of PERT.

NICE guidelines:
The NICE guideline for pancreatitis recommends that people with chronic pancreatitis are offered monitoring of their pancreatic exocrine function and their nutritional status. This should be done at least every 12 months or every 6 months in people under 16. This should be done by clinical assessment and blood tests, to be agreed with a specialist pancreatic centre. Any treatment of vitamin and mineral deficiencies received by the person with PEI should be adjusted according to the results of the assessments. Adults with chronic pancreatitis should also be offered monitoring of their HbA1c level, a test for diabetes, at least every 6 months. Plus, a bone density assessment every two years. Hospital staff should inform GP’s of the need for these assessments.
PEI & diabetes:
People diagnosed with PEI can also develop diabetes. Eight in 10 people with chronic pancreatitis may develop diabetes within 20 years of diagnosis. One in 3 people with cystic fibrosis over 16 years of age will be treated for diabetes. Diabetes can also happen with other causes of PEI but the number of people it affects is unknown.
Symptoms of possible diabetes which should be discussed with your doctor include:
- Unintentional weight loss.
- Feeling very thirsty.
- Peeing more frequently than normal, particularly at night.
- Tiredness.
- Blurred vision.
- Craving sugary drinks and foods.
People with PEI often learn to manage the food they eat to help their symptoms and improve their nutritional status.
Support
What to ask your doctor?
Talk to your doctor if you feel you have PEI or have questions about:
- Your prescribed enzyme medicine dose.
- If you suspect an allergy to your enzymes, for example a skin rash, which is an uncommon reaction.
- If you suspect a medicine side effect, for example, constipation, belly pain, diarrhoea or bloating. Although these side effects can be due to an incorrect inadequate dose.
You will know if your treatment is working as your symptoms of runny poo should improve, pain may be better controlled, and your weight should start to stabilise. PEI might seem complicated but working with your healthcare team it is possible to have a good quality of life with PEI.
References available on request. Contact Guts UK.
About us:
 Guts UK’s vision is of a world where digestive diseases are better understood, better treated and where everyone who lives with one gets the support they need. We fund life-saving research into diseases of the gut, liver and pancreas.
Guts UK’s vision is of a world where digestive diseases are better understood, better treated and where everyone who lives with one gets the support they need. We fund life-saving research into diseases of the gut, liver and pancreas.
Champion our cause; help us fight digestive diseases and change the lives of millions of people in the UK by supporting our work today.
Discover more:






Copyright © 2024 Guts UK. This leaflet was published by Guts UK charity in 2022 and will be reviewed in 2024. The leaflet was written by Guts UK and reviewed by experts in Pancreatic Exocrine Insufficiency and has been subject to both lay and professional review. All content in this leaflet is for information only. The information in this leaflet is not a substitute for professional medical care by a qualified doctor or other healthcare professional. We currently use AI translation tools on our website, which may not always provide perfect translations. Please check for further explanation with your doctor if the information is unclear. ALWAYS check with your doctor if you have any concerns about your health, medical condition or treatment. The publishers are not responsible or liable, directly or indirectly, for any form of damages whatsoever resulting from the use (or misuse) of information contained or implied in this leaflet. Please contact Guts UK if you believe any information in this leaflet is in error.