Overview
This factsheet is about gallstones
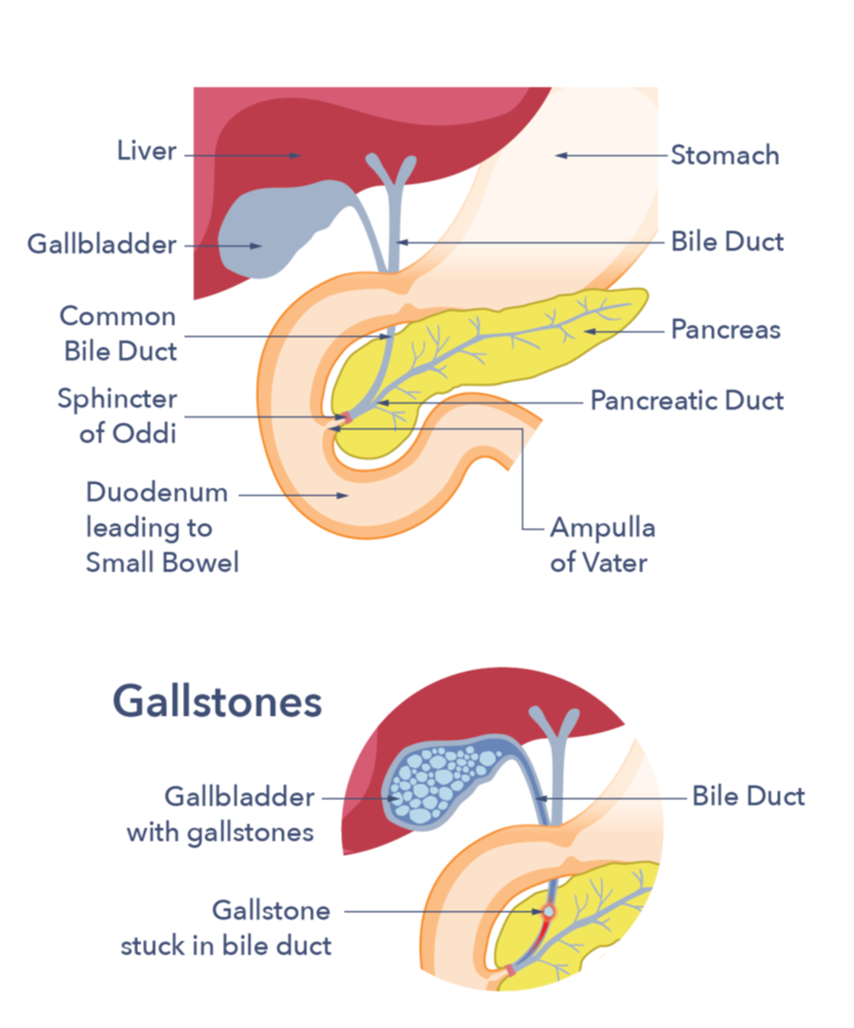
Gall is an old-fashioned word for bile, a liquid made in the liver and stored in the gallbladder. The gallbladder is a small pouch that sits just under the liver. It has the shape of a pear and is about 9 cm long by 4.5 cm wide in size when full. The gallbladder is for storing bile between meals. It fills with bile from the liver between meals, and when we eat the gallbladder empties the bile along a tube (called the cystic duct) into the main bile duct. The bile duct carries bile to the first part of the small bowel immediately after the stomach. Once there, the bile mixes with the food that we have eaten. Bile helps with digestion and absorption, especially of the fats in the food. Gallstones are small, solid lumps that form in bile. They usually cause no symptoms and most people with gallstones are unaware that they have them. However, in some people they can cause problems.
Gallstones affect 10 to 15 people out of every 100 but not everyone will have symptoms. Gallstones are three times more common in women than men. Gallstones happen more often in the gallbladder of females who have an unhealthy high body weight and who have had children. The number of younger females and teenagers who have gallstones is increasing. It is suspected that this is due to changes in the type of diet eaten. Nearly a quarter of females (and a smaller proportion of males) suffer symptoms from gallstones by the age of 60. The risk of developing symptoms increases with age.
Causes
How do gallstones occur?
Bile is made up of a mixture of different chemicals. Gallstones form when bile becomes so concentrated that the chemicals can no longer stay dissolved. Gallstones begin as tiny crystals, grow to resemble gravel, and can eventually grow to the size of pebbles. The crystals form as the proportion of substances in liquid bile changes. There are two types of gallstones.
The first type of gallstones is formed from cholesterol and is more common. Bile is high in cholesterol, a fatty substance that is important for health but when present in excess can cause heart disease. In fact, bile is one way the body rids itself of excess cholesterol. Bile, on the other hand, may have so much cholesterol that when it is stored in the gallbladder, the cholesterol separates as small crystals. These crystals may combine to form a gallstone.
Pigment stones, the second type of gallstone, are found in around 3 out of every 10 people with gallstones. Bilirubin, a waste product from the turnover of red blood cells is excreted by the liver into bile and under some circumstances can form pigment stones in the gallbladder. The type of stone that forms is determined by a person’s lifestyle, ethnicity, and medical history. Some gallstones can be mixed.
Sometimes, there is just a single stone in the gallbladder. But often there are several, and in rare cases there may be literally dozens of small stones. Although the size and quantity of stones typically do not determine whether a person will experience issues, they can determine which complications may occur (see below).
What are the causes?
There are many risk factors that have been linked to gallstone disease. Examples of this include becoming older, being a female, and having a close family member who has gallstones. Additionally, those people with inflammatory bowel disease or people who have undergone a period of fast weight loss of more than 1.5 kg each week, are more likely to develop gallstones. However, for people who are overweight the health advantages of weight loss far overweigh the risk of gallstones. Gallstones can also form in people who have had weight loss surgery. The risk is also higher with increasing waist measurement, which is an indicator of abdominal (tummy) fat, even among people who have a healthy weight.
People with the hereditary conditions sickle cell disease and hereditary spherocytosis have an increased risk of developing gallstones and in these conditions, gallstones may run in families.
Symptoms
What are the usual symptoms?
About two out of every three people who have gallstones have no symptoms and are usually unaware they have them. Gallstones are occasionally discovered by accident when investigating another condition, in which case they are usually not treated. Gallstones typically only cause symptoms if the gallbladder becomes inflamed or if the stones travel from the gallbladder into one of the bile ducts. The ducts connect the liver, gallbladder and small bowel. Possible complications include:
Biliary colic: If the gallstones get stuck in the narrow neck of the gallbladder or in the bile duct that drains the gallbladder, this can cause pain called biliary colic. The pain can be severe and is described as a cramping pain that is felt in the top of the stomach (belly). It is most usually felt either in the middle of, or just under the ribs on the right-hand side. The pain can go around to the back and to the right shoulder. It is generally a continuous pain but may come in waves. It is usually rather more severe than ‘indigestion’ and could be described as severe heartburn.
It is not uncommon for the person with gallstones to feel so uncomfortable that they may seek medical advice. The pain usually lasts for several minutes to a few hours. Occasionally, people with gallstone pain may feel sick or even vomit. The pain often follows a meal and may be noticed most often in the evenings. However, it may occur at any time. Biliary colic is the most common symptom of gallstones.
Cholecystitis: The stones may cause inflammation in the wall of the gallbladder, known as cholecystitis. This also causes pain like biliary colic, but it doesn’t go away without medical intervention. The area on the top right of the abdomen can also get very tender to touch. People can feel very sick and flu-like, and even develop sepsis (a widespread infection).
Jaundice (sometimes called yellow jaundice): Bilirubin is a yellow-green chemical that occurs normally in the body. If a gallstone blocks the main duct leading from the liver into the bowel, bilirubin can’t be removed from the body and a yellow colour can be seen in the eyes and skin. People with a darker complexion may find it more difficult to detect changes in skin colour. Bilirubin comes from red blood cells that have been processed at the end of their natural life. It is one of the body’s waste products that the liver deals with by mixing it with bile. Some pigment does escape into the urine, making it look a very dark colour, while poo can be very pale.
Cholangitis: If the stone doesn’t pass and remains stuck in the bile duct it can cause a serious condition called cholangitis which occurs when the blocked bile becomes infected. If this happens the person becomes feverish and often develops shivering. This is a medical emergency.
Diagnosis
HOW ARE GALLSTONES DIAGNOSED?
If a person complains of pains anywhere around the top of the belly (abdomen), especially if these pains have been lingering for a few hours at a time and coming and going in waves, the doctor may suspect gallstones. The presence of jaundice adds to the likelihood of gallstones and should always be checked out thoroughly. A visual check for signs of jaundice would be carried out, and often blood tests would be sent away. In addition, the doctor will carry out a physical examination to determine whether there is soreness at the top of the abdomen. If these findings point to a diagnosis of gallstones, it is usual for the person with symptoms to be referred for further investigations. These can include:
- Blood tests: These will be carried out to determine whether there are signs of jaundice or inflammation.
- Ultrasound scan: This is where a small flat device is moved over the upper belly (abdomen) in the region of the liver and gallbladder. Most gallstones reflect ultrasound very well. Unless they are deep in the abdomen or hidden behind some gas in the bowel, they are easily detected on the screen. It is important to not eat or drink before having this scan to make sure the gallbladder is as full of bile as possible.
- CT or MRI scan: If the ultrasound scan does not give a clear result, other tests may be needed such as a CT or MRI scan.
Treatment
WHAT TREATMENT IS AVAILABLE?
If the gallstones are not causing any symptoms, then it is not necessary to have any treatment at all. Even if you have one attack of pain from gallstones, there may be no further trouble for many years, if ever. Even if a gallstone has travelled out of the gallbladder down the bile duct, most will pass into the small bowel and be passed naturally. In effect, the person with gallstones has cured themselves of the problem.
If gallstones are causing recurring pain or have caused complications, then they can be removed. This is usually done by surgery to remove the gallbladder with the gallstones in it. Other techniques can be used to remove gallstones that have escaped from the gallbladder:
Surgery: If the gallstones are all contained in the gallbladder, then the simplest method is to have an operation to remove the gallbladder. This is called a called a cholecystectomy. Surgery also removes the stones within it. Nowadays, this is usually done via keyhole surgery (laparoscopic surgery), a procedure that most people can have done as a day case. This is a huge improvement from the much larger operations that were necessary for gallstones in the past. However, every operation carries risks and should not be entered into lightly. There is no question that, for most people, keyhole surgery is currently the best option for treating gallstones.
Gallbladder surgery is generally considered safe and effective and causes no problems for most people who have it. However, you should always ask your surgeon about the benefits of surgery and risk of complications. Remember that any risks should be weighed up against the risks of not having surgery. A proportion of people (around 13 in 100) may develop diarrhoea after gallbladder surgery, and this may not come on until up to 3 months after the operation. Importantly, if diarrhoea persists, then people should be investigated for a condition bile acid diarrhoea (BAD). This is sometimes referred to as “bile acid malabsorption”. BAD is more frequently seen in young women and men over the age of 50. BAD is readily treatable if it is recognised so if you develop diarrhoea within 3 months of your operation make sure to discuss it with your doctor.
Surgery may very occasionally cause damage to the bile ducts (up to 1 in 200 chance) and rarely a stone may get stuck in the ducts during surgery (this happens in 1 in 100 people). Other rare complications include damage to the pancreas, (an organ that sits close to the gall bladder) resulting in pancreatitis; infection; and bleeding. Any symptoms after surgery should therefore be reported to your doctor.
It should be remembered that most surgical complications are a rare occurrence.
Endoscopic Retrograde Cholangio-Pancreatography (ERCP): This is where stones in the bile duct are removed with a flexible endoscope. With ERCP, the endoscope is passed through the mouth, down to the stomach, to reach the opening of the bile duct into the bowel. A tiny tube is then passed through the endoscope and inserted into the lower end of the bile duct. Initially, a dye is squirted through this tube so that an x-ray picture of the duct can then be taken. This is called a cholangiogram. If the cholangiogram confirms the presence of a stone in the duct, this can either be removed directly or the bottom end of the duct can be enlarged to allow the stone to pass out naturally. Alternatively, small drainage tubes (stents) may be inserted around the stones to allow the bile to flow freely again. These techniques mean that an operation can be avoided. This is useful for frailer people with gallstones in the bile duct, who may not be able to have surgery. ERCP has a small risk of quite serious complications, including pancreatitis (around 1 in 50) and serious bleeding (around 1 in 100), so it should be carefully considered.
Shock Waves: At some specialist centres, large gallstones that are otherwise difficult to treat can be broken up by using shock waves.
Abscess caused by an infection in the gallbladder (gallbladder empyema).
This is a build-up of pus that occasionally happens with a blocked gallbladder. If symptoms do not settle and surgery cannot take place, the pus would need to be drained. It is done by inserting a tube through the skin to where the infection is (percutaneous cholecystostomy). Once the infection settles, then surgery or endoscopy treatment may be considered.
Do gallstones need to be monitored, and if so, how?
There is some variation in the treatment of gallstones. Some people are offered treatment for symptomless gallstones to prevent problems in the future. This is especially the case if they have had acute pancreatitis caused by gallstones. Other people can be safely helped by a watch-and-wait approach. When people have symptoms, they should be offered treatment, so please contact your GP if symptoms occur. While waiting for treatment, it is advisable to avoid any foods that cause symptoms. Dietary tolerance varies between individuals, and sometimes having smaller meals more regularly through the day can be helpful. There is no research to suggest that either gluten free or dairy free diets are helpful for gallstone symptoms, so these diets won’t help. If you lose weight or struggle to eat, please contact your GP immediately.
What about after gallbladder removal?
The operation to remove the gallbladder is extremely common, with more than 60,000 performed on the NHS every year. The gallbladder, while useful, is not essential to the body. Its removal should raise no problems and you can live perfectly well without a gallbladder. If there is no gallbladder, bile just passes continuously into the bowel, rather than being stored between meals. There is no problem with digestion, and most people do not have any longer-term after-effects from having their gallbladder removed. However, in some people their original symptoms persist or recur after treatment. If this is the case, it is quite possible that the original symptoms were not due to the gallstones.
Ordinarily, if you have no symptoms, there is no need to continue to alter your diet after treatment. You may see information on the Internet suggesting that having the gallbladder removed causes a low level of bile. This is not correct; the liver produces the same level of bile as it did before the surgery. Bile supplements are therefore not needed.
If you have continuing symptoms, then these should be reported to your GP so the cause can be identified, and treatment offered. It is important to consider testing for bile acid diarrhoea, if diarrhoea is a symptom. Sometimes other conditions, such as irritable bowel syndrome (IBS) can cause pains that seem to be coming from the gallbladder, and these symptoms will not improve after a cholecystectomy. However, there are treatments available for IBS if it is diagnosed.
It is important to note that people who are at high risk of stone formation may, after some time, develop further stones in the bile ducts. They will potentially suffer symptoms again. If this happens the person with gallstones is usually offered an ERCP.
Support
What to ask your doctor?
- I am getting stomach pains – have I got gallstones?
- I think I have gallstones, what should I do?
- Will diagnosis be uncomfortable for me?
- Are gallstones dangerous?
- What are the risks and benefits of the treatment?
References are available on request.



