Acute pancreatitis
Download printable versionOverview
This factsheet is about acute pancreatitis
Acute pancreatitis occurs when the pancreas is damaged resulting in the release of the digestive enzymes into the pancreas. It occurs in 34 per 100,000 people every year.
Although pancreatitis typically affects people in their middle or later years, it can occur at any age, including childhood. It affects both men and women.
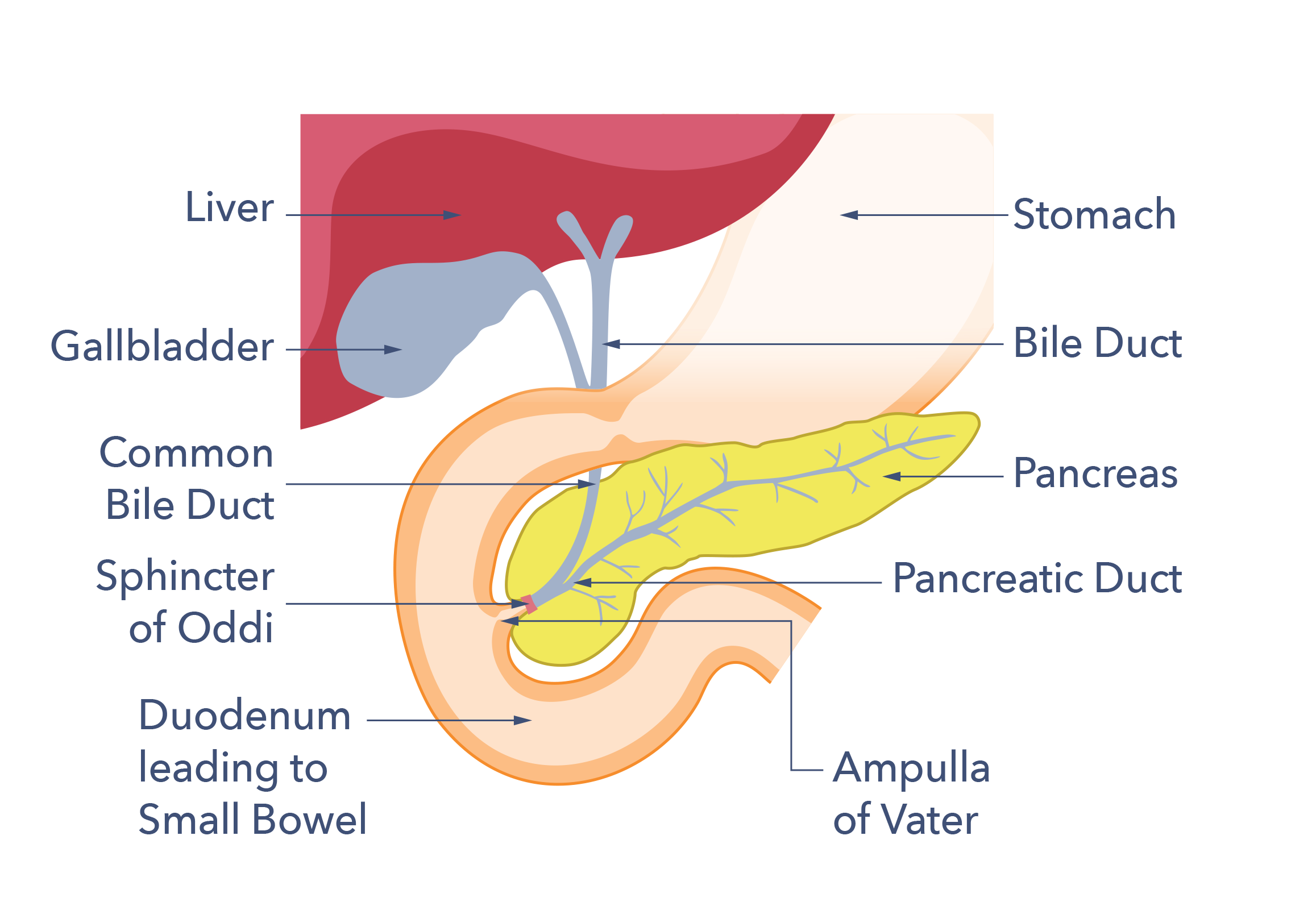
What is the pancreas?
The pancreas is a gland which secretes enzymes and hormones. It is located in the top portion of the abdomen, in front of the spine and behind the stomach. It is around 25cm (nine inches) long, salmon pink in colour, and at its widest point is about the thickness of your wrist.
The pancreas has two main functions. One is to secrete digestive enzymes, which enter the small intestine via the pancreatic duct to help your body digest food. The second is the production of hormones including insulin, which regulate the body’s total energy resources and blood sugar levels.
79 out of 100 adults who develop acute pancreatitis fully recover and never have another episode.
What is acute pancreatitis?
Acute pancreatitis occurs when the pancreas is damaged, resulting in the release of the digestive enzymes into the pancreas. This causes severe inflammation and death of the pancreas tissue. Normally, the digestive enzymes are secreted into the small bowel where a protective “chemical cap” is removed. This allows enzymes to digest food. If they start working too soon, the pancreas becomes red, inflamed and swollen and may suffer irreversible damage. In severe disease, large parts of the organ die and this is called necrotising pancreatitis.
Acute pancreatitis occurs in 34 per 100,000 people every year. Although pancreatitis typically affects people in their middle or later years, it can occur at any age, including childhood, and affects both men and women. 1 in 4 people who experience an acute pancreatitis attack may experience problems with other organs, particularly kidney failure and lung damage. This is a particular risk for people with severe necrotising pancreatitis. When this happens, people may need care in an intensive care unit (ICU) or high dependency unit (HDU). It is unclear why some people experience these complications and others don’t. We need better tests to determine early which people are going to have symptoms. This is so treatment can be started as soon as possible.
The long-term damage that results from pancreatitis is unpredictable. Although the damage may be minor and short lived, in others it may be severe causing longer lasting symptoms. 79 out of 100 adults who develop acute pancreatitis fully recover and never have another episode. However, those who need high dependency or intensive care treatment may experience longer lasting problems because of permanent damage to the pancreas. Examples include chronic pancreatitis, where the inflammation persists, and problems related to a failure of the pancreas to function occur. This includes pancreatic exocrine insufficiency (PEI). In PEI the pancreas loses its capacity to secrete the digestive enzymes. Diabetes can occur when insulin producing cells are destroyed or fail to recover. Adults will experience another case of acute pancreatitis in 21 out of 100 cases. This is called recurrent pancreatitis and 8 in 100 adults with recurrent pancreatitis go on to develop long-term or chronic pancreatitis.
Causes
What are the causes of acute pancreatitis?
Pancreatitis in adults
8 in 10 cases of pancreatitis in adults are caused by either gallstones or excessive alcohol consumption. Gallstones are the most frequent cause of acute pancreatitis. The second most frequent is drinking alcohol above recommended limits. Gallstones cause problems when small stones pass out of the gallbladder into the bile duct and block the duct that drains the pancreas. This blockage can be short term, if the stone is expelled, but if the stone becomes stuck, the damage persists. Treatments may be needed to remove the stone and relieve the blockage. The longer the delay is in relieving the blockage, the more severe the damage to the pancreas.
Alcohol damages the pancreas. Some people are more susceptible to alcohol damaging the pancreas because of their genetic make-up. Sometimes this results in pancreatitis running in families. Damage occurs both with drinking too much in a short time (binge drinking) and regular excessive drinking. Smoking tobacco is also thought to be toxic to the pancreas and this is another contributory factor in the risk of developing pancreatitis.
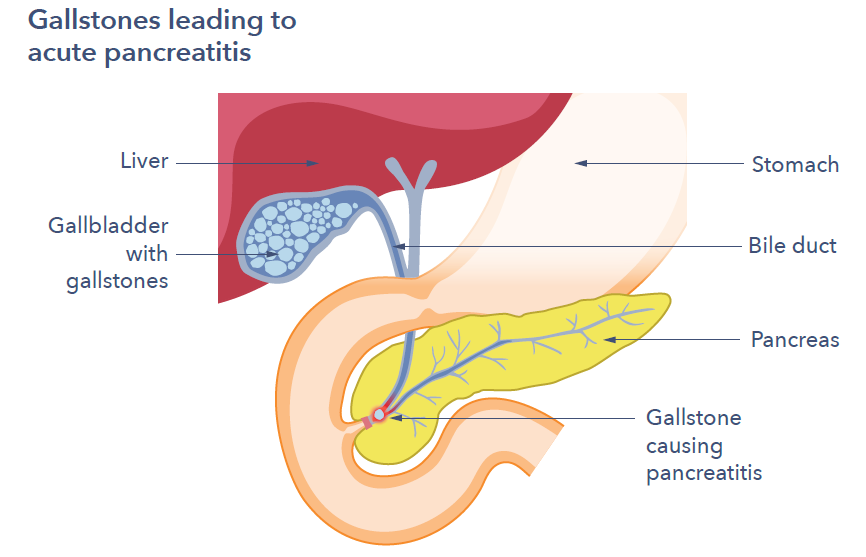
Gallstones leading to acute pancreatitis
1 in 10 people who experience acute pancreatitis, no known cause can be found, this is called idiopathic pancreatitis. For the remaining 1 in 10 cases, pancreatitis episodes have unusual causes, such as:
- Following trauma, for example, a road traffic or bike accident.
- As a rare side effect of some medicines, such as azathioprine and steroids.
- Genetic problems that lead to too much fat in the bloodstream (known as
hypertriglyceridemia). Familial Chylomicronaemia Syndrome, is a group of
conditions that run in families and lead to high levels of triglycerides, a type
of fat, in the body. - A high level of calcium in the blood (hypercalcaemia).
- As part of an autoimmune disease (when the body’s immune system, which has evolved to fight infections turns on itself).
- If the duct draining the pancreas gets blocked by a cancerous growth.
- Following a medical procedure called endoscopic retrograde cholangiopancreatography (ERCP) in which the bile duct or pancreatic duct are investigated. This occurs in less than 5 in 100.
- Some viral infections, including Covid-19.
1 in 10 individuals are born with an anomaly in the ducts that drain the pancreas. This is called pancreas divisum and is associated with a small increased risk of developing pancreatitis. Most people with pancreatic divisum do not experience any problems.
Pancreatitis in pregnancy is rare, happening in fewer than 1 in 1,000 to 1 in 12,000 pregnancies. When it does occur, it is usually caused by gallstones or elevations in blood triglyceride (fat) levels. Pancreatitis generally occurs late, typically in the third trimester.
Pancreatitis in children
Pancreatitis in children is rare, occurring in less than 1 in 10,000 children. Gallstones and medicines are the main causes. In some children a cause cannot be found and the pancreatitis is classified as idiopathic pancreatitis. A minority of children with pancreatitis go on to have further episodes, especially those with genetic causes. Reports have suggested that pancreatitis is more common in children from a Pakistani ethnic background, but these figures need confirming.
How can acute pancreatitis affect you?
Acute pancreatitis can be very painful and may require a hospital stay. Most people achieve a full recovery, although this may take some time. Some will suffer from recurrent attacks and a small number may have persistent or chronic pancreatitis.

1 in 10 people who experience acute pancreatitis, no known cause can be found, this is called idiopathic pancreatitis
Symptoms
What are the usual symptoms of acute pancreatitis?
People experience:
- A sudden onset of abdominal (belly) pain, usually starting in the upper abdomen developing over minutes to hours.
- Pain that can also travel through to the back.
- Feeling sick (nausea) and being sick (vomiting).
- A fever and a high heart rate particularly in severe disease.
Most people need to be admitted to hospital to control the pain and start treatment.
How is acute pancreatitis diagnosed?
Diagnosis is based on the symptoms experienced and a positive blood test for enzymes produced by the pancreas (called amylase and lipase). These enzymes are not normally detectable in the blood. But in response to injury to the pancreas they are released and spill over into the blood. This test is only available in hospital and mild pancreatitis might not show a positive blood test. Sometimes, the early diagnosis of acute pancreatitis is not clear. In such cases, a special X-ray called a CT or MRI scan can be useful in making the diagnosis. A CT scan is often also done to assess the extent of the damage to the pancreas. It can also rule out other possible causes of pain if the diagnosis is not clear.
Everyone with acute pancreatitis should have an ultrasound scan to check for gallstones as a possible cause. The ultrasound doesn’t need to be done as an emergency and can be done in the first few days.
How can acute pancreatitis affect me overtime?
People with pancreatitis typically stay in the hospital for 5 to 10 days. If the pancreatitis is severe and complications develop, people can be in hospital for several months. For people that achieve a full recovery at home, their recovery can be up to three times the length of a hospital stay.
For people who need treatment on an intensive care unit, this can be a traumatic experience with long-term effects on mental and physical health. If you feel this has happened, talk to your doctor about what help is available. Talking to others through support groups and family members can also help.
Some people develop complications around the pancreas, particularly the formation of fluid-filled collections called cysts. If this happens, recovery may take longer, and further treatment is sometimes required.
Most people achieve full recovery, although some will suffer from recurrent attacks. A small number may have persistent or chronic pancreatitis. If the damage is severe, people may need supplementary digestive enzymes to help to digest food. About 1 in 5 adults who have had severe acute pancreatitis will go on to develop diabetes in the future.
Symptoms which suggest the development of diabetes and should be discussed with your doctor include:
 Unintentional weight loss.
Unintentional weight loss.- Feeling very thirsty.
- Peeing more often than normal, particularly at night.
- Craving sugary drinks and foods.
- Other symptoms might include tiredness and blurred vision.

Everyone with acute pancreatitis should have an ultrasound scan to check for gallstones as a possible cause.
Treatments
What treatment is available for acute pancreatitis?
There is no current medicine or treatment that can stop the inflammation in acute pancreatitis. Guts UK is funding research aiming to understand the inflammation that occurs during pancreatitis better. We are dedicated to finding an effective treatment for pancreatitis. Supportive treatments such as fluids through a drip and oxygen delivered through a mask are often needed. In more severe cases, a bladder catheter may be inserted to check urine output and a slender naso-gastric tube passed via the nostril into the stomach. This tube allows extra feeding to be given.
The abdominal pain can be extreme requiring strong painkillers including morphine-type drugs. Although antibiotics can sometimes be necessary to treat complications, they are not routinely used because pancreatitis is not an infection.
Often people get better quickly and can eat and drink within a few days, but sometimes longer-term tube-feeding is needed. Most people have only mild inflammation and soon settle, but some develop complications. These complications may require specialist interventions using endoscopy or surgery.
Rarely a telescope examination called an ERCP is needed. The reasons this might be required are:
- If there is an infection in the bile duct (cholangitis)
- If there is a stone jammed in the bile duct blocking the pancreas duct.
ERCP is used to remove the blockage and drain the ducts. Your healthcare team will discuss treatment with you and will advise what and when treatments should be given.
Once people are over the worst part of the attack, it is very important to search for and treat any underlying cause of the pancreatitis. For example, if gallstones are the cause they can be removed by surgery. This is usually done soon after the attack has settled to prevent more attacks in the future.
If the cause of acute pancreatitis is alcohol, it is really important that the person with pancreatitis stops drinking alcohol completely and forever. This may require specialised help, as it can be difficult to do it alone. Ask your doctor about alcohol services in your area. If you have another cause of pancreatitis that recurs or becomes chronic, you should stop drinking alcohol permanently. Alcohol can aggravate pancreatitis caused by other conditions.
People are also recommended to stop smoking because tobacco and nicotine are thought to be toxic to the pancreas. Help is available, most NHS services include a stopping smoking service. Asking for professional help can boost your chances of being successful.
Probiotics are not effective for treating pancreatitis. In some studies their use has been associated with a worse outcome so they should not be used.
Who treats pancreatitis?
People in hospital with pancreatitis are treated by a multi-disciplinary team (MDT). The team may include a doctor who specialises in gastroenterology (diseases of the gut, liver and pancreas), a surgeon, nurses, pain management team and a dietitian.
For those who are in hospital for some months and lose fitness, rehabilitation with a physiotherapist or occupational therapist may be needed. If someone has been on a life support machine with a breathing tube, once in a while swallowing function takes time to recover. A speech and language therapist might be needed to give advice about correct food and drink textures to have, whilst swallowing improves.
For people who experience complications of pancreatitis, the MDT may consult a specialist hepato-biliary (related to liver and gallbladder) centre if this service is not available through the hospital. These centres are regional hospitals that have specialist teams that provide advice and/or treatment to peoples with pancreatitis. Children will be treated with a paediatric (specialist children’s) team, containing similar healthcare practitioners as above, but who treat children specifically.
For relatives visiting someone with severe pancreatitis on the intensive care unit, it can be upsetting to see all the machines used. The staff can explain what the machines are for and how they are helping your relative.
What complications can occur?
In the first week, the main complications arise if severe pancreatitis triggers whole-body inflammation, affecting other organs. This can lead to low blood pressure and a rapid heart rate. This situation requires specialist care on an ICU or HDU to control the blood pressure with the use of fluids given through a vein and medicines to increase blood pressure. If the lungs are affected, breathing problems may require oxygen supplementation. This is given through a mask. Or in very severe cases, by putting the person to sleep and supporting their lungs on a ventilator and life support machine.
Fluid can collect around the pancreas and sometimes pockets of fluid called pseudocysts can form. Sometimes these fluid collections can become infected and need antibiotics given through a drip. Most of these settle on their own but sometimes they need to be drained. The pseudocyst is drained using a needle or drain inserted through the side of the belly, or via endoscopy or rarely a surgical operation. If parts of the pancreas or surrounding tissues die during the attack, they can get infected and turn into an abscess that also may need to be drained. These treatments are usually performed in a specialist pancreas centre. Your doctor can advise you about the treatment plans.
Unfortunately, acute pancreatitis can be so extreme that some people die. Overall,1 in 15 to 1 in 20 people who experience severe acute pancreatitis will die from that attack. Nearly all deaths from acute pancreatitis occur in those people who needed to go to high-dependency or intensive care. Deaths amongst children are rare.

Once people are over the worst part of the attack, it is very important to search for and treat any underlying cause of the pancreatitis.
Support
What to ask your doctor?
 Will my pancreatitis go away?
Will my pancreatitis go away?- Should I be monitored after leaving hospital?
- What signs of sickness should I look out for when I am discharged from hospital that mean I might need to a see specialist or need to be readmitted?
- If gallstones were the cause of my pancreatitis, when will I have my gallbladder removed?
- Where is my local pancreas centre?
- When does acute pancreatitis become chronic?
- Do I need prescription digestive enzymes? What diet is best? (Ask your dietitian.)
- Do I need testing for diabetes?
For adults and children that are diagnosed with hereditary pancreatitis, if they and their family wish, there is the possibility of being referred for genetic testing. This will involve a discussion with a genetic counsellor about the impact that this testing may have on the individual and the family. Your hospital specialist can refer you.

For adults and children that are diagnosed with hereditary pancreatitis, if they and their family wish, there is the possibility of being referred for genetic testing.
Research
Your priorities for pancreatitis research
At the beginning of 2021, Guts UK started the process of identifying the top 10 research priorities for pancreatitis in the UK. It was important to us that patients, their families, carers and healthcare professionals decided this top 10 together, with equal voices. Now, in November 2022, we are delighted to announce your top 10 research priorities for acute and chronic pancreatitis, in both children and adults.
NICE guidelines on pancreatitis:
The NICE guidelines on pancreatitis aim to improve the quality of care, information provision and support for people with pancreatitis. The guidelines have a section on information to the public, explaining the care that people with pancreatitis should expect.
The future looks brighter. This is the first time you have been asked what research you’d like to see into your condition. Now, Guts UK is working hard to promoting these questions and putting them questions into ‘researchable’ format. We’re dedicated to finding an effective treatment, a cure for pancreatitis.
 The National Institution of Health & Research (NIHR) allocate more research funding for conditions with PSPs, which we’re delighted to say that pancreatitis now has! Researchers applying for grants within the top 10 priority areas are more likely to be successful.
The National Institution of Health & Research (NIHR) allocate more research funding for conditions with PSPs, which we’re delighted to say that pancreatitis now has! Researchers applying for grants within the top 10 priority areas are more likely to be successful.
We finally have a direction for pancreatitis in the UK, a condition that has been neglected and misunderstood for too long. Together, we’re changing that. Thank you.
Your top ten research priorities for pancreatitis!Your kindness helps us to fund life-saving and life-changing research. Helping us to shape and change the future for those with pancreatitis.
Our current active research into pancreatitis
Dr Kattakayam is assessing whether protecting the mitochondria (cell powerhouses) outside of the pancreas cells (within other cells and organs), reduces the severity of the condition and prevents worsening damage to the pancreas itself.
is assessing whether protecting the mitochondria (cell powerhouses) outside of the pancreas cells (within other cells and organs), reduces the severity of the condition and prevents worsening damage to the pancreas itself.
Guts UK is the only UK charity funding a research fellowship into pancreatitis. We are dedicated to finding an effective treatment, a cure, for this devastating disease.
Please donate today, to help us fund more research, reach more people and empower people to seek help. ABOUT US:
ABOUT US:
Guts UK is the only charity in the UK funding a research fellowship into pancreatitis. We’re dedicated to finding an effective treatment for this disease.
Each November, we hold a month-long pancreatitis awareness campaign: Kranky Panky.
Join our community, champion our cause and help us fight pancreatitis. If you’re feeling inspired but don’t know how best you can help, read some fundraising ideas here or contact team Guts UK today – we’d be delighted to lend a hand.
DISCOVER MORE:




This information was published by Guts UK in 2023 and will be reviewed in 2025. The information was written by Guts UK and reviewed by experts in Acute Pancreatitis and has been subject to both lay and professional review. All content on this page is for information only and is based on the UK health system. The information on this page is not a substitute for professional medical care by a qualified doctor or other healthcare professional. ALWAYS check with your doctor if you have concerns about your health, medical condition, or treatment. The publishers are not responsible or liable, directly, or indirectly for any form of damages whatsoever resulting from the use (or misuse) of information contained or implied by this information. Please contact Guts UK if you believe this information is in error.